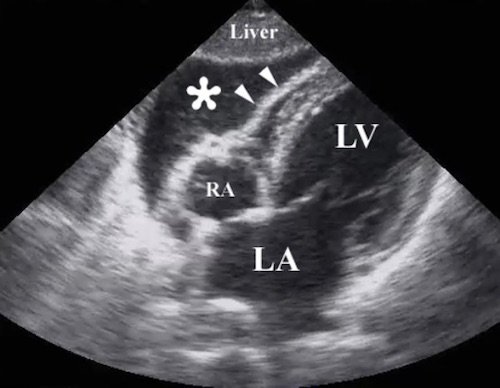
FAST: Pericardial Window (Positive) 1
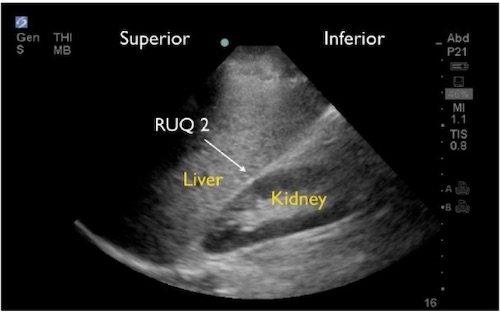
FAST: Perihepatic Window 2
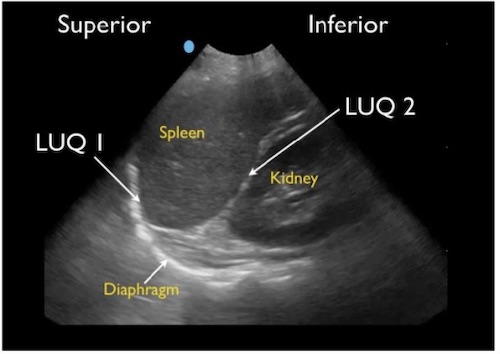
FAST: Perisplenic Window 2
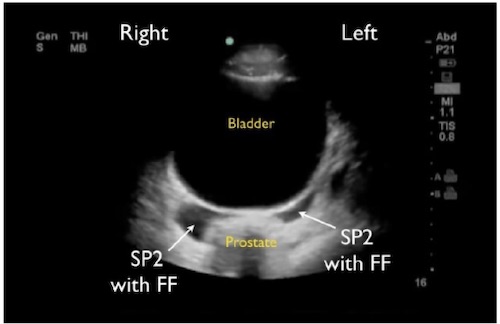
FAST: Pelvic Window (Positive) 2
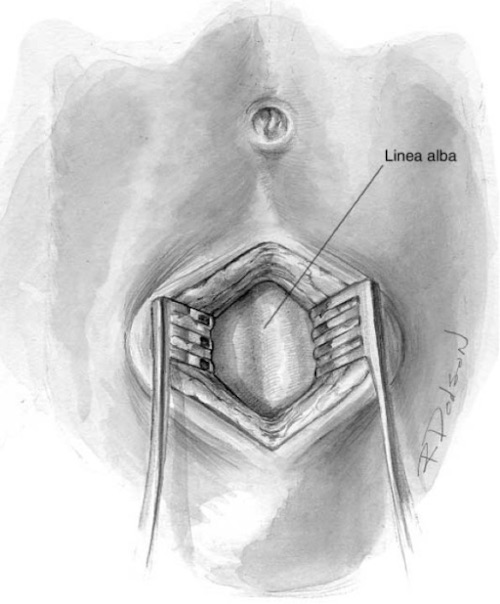
DPL: Expose Linea Alba 3
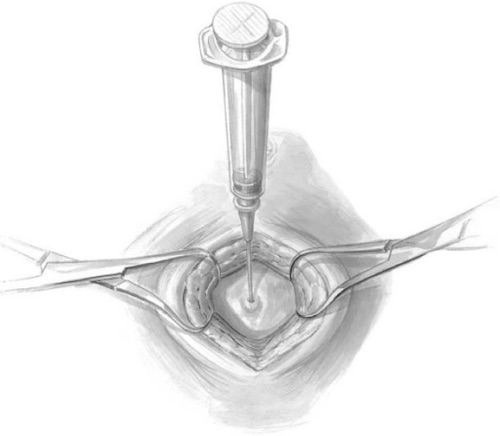
DPL: Access the Peritoneal Cavity 3
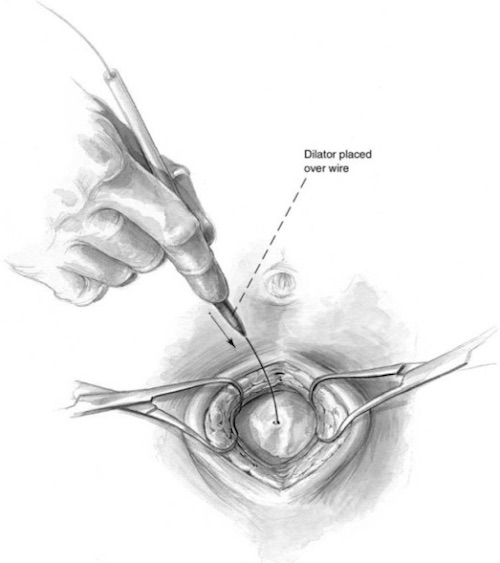
DPL: Place Catheter Over a Guidewire 3
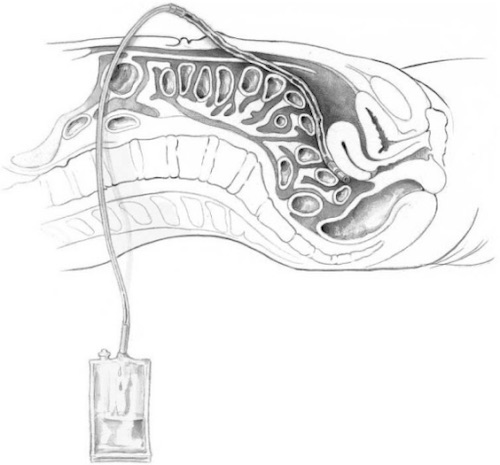
DPL: Instill Fluid & Collect Back 3