Acute Colonic Pseudoobstruction (Ogilvie Syndrome/ACPO)
Acute Colonic Pseudoobstruction (Ogilvie Syndrome/ACPO)
Laura Lynn Beck, MD and David Ray Velez, MD
Table of Contents
Definition
Definition: Acute Colonic Dilation in the Absence of Mechanical Obstruction
Mortality Risk: 8% (40-45% if Perforated)
Etiology
Most Commonly Presents in Elderly Hospitalized Postoperative Patients with Comorbid Conditions
Medications
- Opiates – Most Commonly Associated Medication
- Anticholinergics
- Dopaminergic Agents
- Alpha-Adrenergic Agents
- Calcium Channel Blockers
- Antipsychotics
- Cytotoxic Agents
- Epidural Anesthesia
Surgery
- Orthopedic Surgery – Particularly Hip Surgery
- Spine Surgery
- Pelvic Surgery
- Cesarean Section
- Cardiothoracic Surgery
Additional Risk Factors
- Elderly
- Dementia
- Stoke
- Malignancy
- Infection
- Myocardial Infarction
- Heart Failure
- Trauma
- Electrolyte Imbalances
- Hypokalemia
- Hypocalcemia
- Hypomagnesemia
Presentation and Diagnosis
Presentation
- Abdominal Distention – Primary Clinical Feature
- Abdominal Pain
- Nausea and Vomiting
- Constipation (51%) or Diarrhea (41%)
Symptoms Have an Average Onset 5 Days Postoperatively
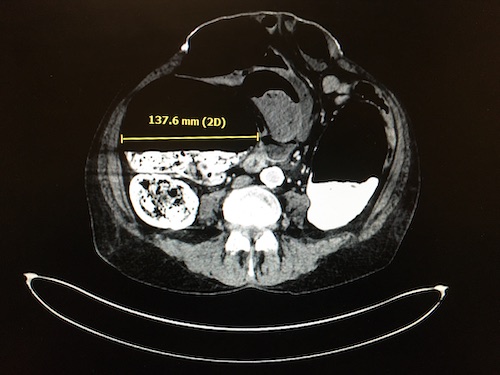
Diagnosis: Made by CT Abdomen/Pelvis
- Demonstrates Proximal Dilation Extending from the Cecum with No Mechanical Source of Obstruction
- Extends to:
- Hepatic Flexure: 17%
- Splenic Flexure: 56% (Most Common)
- Left Colon: 27%
- Colon Wall Thickness is Usually Normal – Wall Thickening Raises Concern for Ischemia or Toxic Megacolon
- Consider Repeat CT with Water-Soluble Rectal Contrast if Obstruction Remains Unclear
Important to Rule Out Mechanical Large Bowel Obstruction and Toxic Megacolon in Diagnostic Evaluation
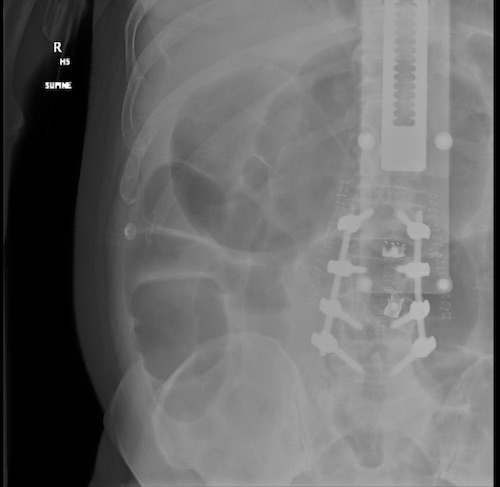
Can Monitor with Abdominal Plain Film (But Not Specific for Diagnosis)
High-Risk for Perforation if the Cecum is Dilated > 10-12 cm or if Duration is > 6 Days
Acute Colonic Pseudoobstruction
Acute Colonic Pseudoobstruction
Management
The Primary Goal of Management is to Decompress the Colon to Prevent Ischemia and Perforation
Cecum Diameter < 10-12 cm: Initial Trial of Conservative Management and Bowel Rest
- Fluid Resuscitation
- Correct Any Electrolyte Derangements
- Discontinue Any Contributing Medications
- Serial Abdominal Exams
- Serial Abdominal Plain Films Every 24 Hours
- Success Rate: 70-90%
Cecum Diameter > 10-12 cm, Severe Abdominal Pain, or Failure of Conservative Management After 48-72 Hours: Neostigmine
- *See Use and Contraindications/Complications Below
- Success Rate: 85-90%
- Consider a Second Dose of Neostigmine After 24 Hours
If Neostigmine Contraindicated or Fails: Endoscopic Decompression
- Endoscopy Done without Prep or Insufflation – Risk for Aspiration or Perforation
- Extensively Suction Air Once the Most Proximal Extent Accessible is Reached
- Consider Leaving a Decompression Tube to the Cecum or Transverse Colon for Continued Decompression (Decreases the Risk of Recurrence)
Surgical Intervention
- Indications:
- Failure of Medical Management (Neostigmine and Colonoscopic Decompression)
- Ischemia
- Perforation
- Peritonitis
- Surgery Generally Consists of Cecostomy/Colostomy and/or Resection as Indicated
Cecostomy Tube
- May Be Considered for Patients Who Fail Medical Management (Neostigmine and Colonoscopic Decompression) as an Alternative to Surgery
- Can Be Performed Percutaneously by Endoscopy or Interventional Radiology
- May Be Safe and Effective for Select Patients but Less Well Validated and Can Be Complicated Infection, Bleeding, and Bowel Perforation/Peritonitis
Neostigmine: Use and Contraindications/Complications
Mechanism of Action: Acetylcholinesterase Inhibitor
Dose: 2-5 mg IV Gevin Slowly Over 5 Minutes
Contraindications:
- Recent Myocardial Infarction
- Asthma
- Bradycardia
- Hypotension
- Acidosis
- Beta-Blocker Therapy
Complications:
- Bradycardia [6%]
- Hypotension
- Bronchospasm
- Seizure
- Sialorrhea
- Diarrhea
- Nausea
- Abdominal Pain
Give in a “Monitored Setting” to Monitor for Complications
- Keep Atropine at Bedside for Bradycardia