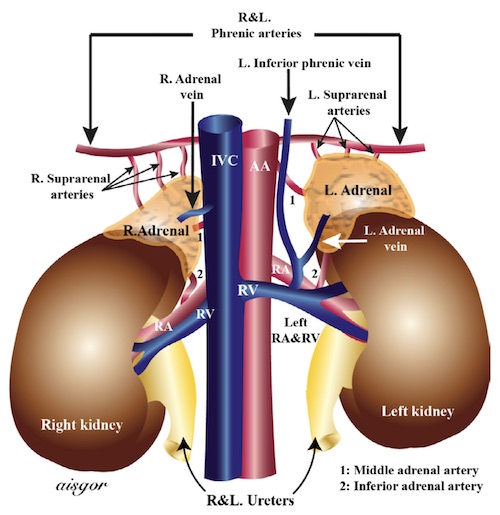
Adrenal Vasculature 1
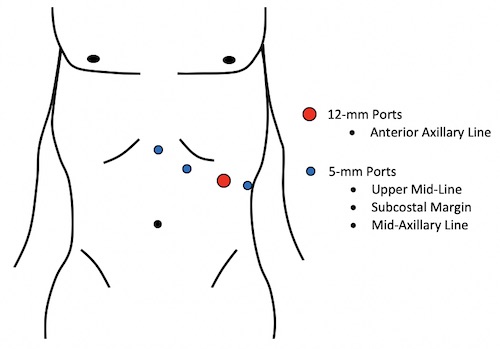
Left Laparoscopic Adrenalectomy Port Placement
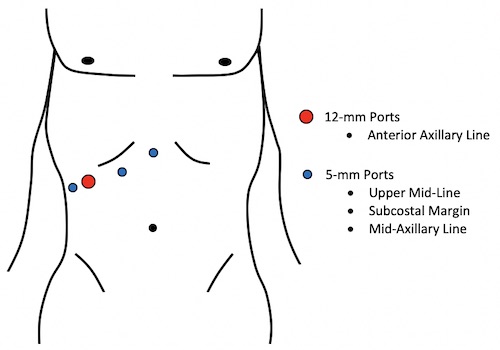
Right Laparoscopic Adrenalectomy Port Placement
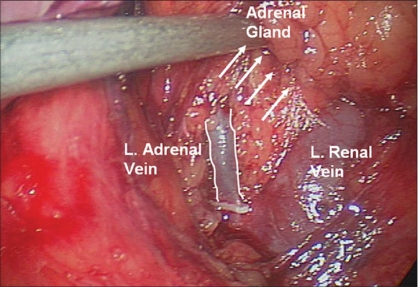
Left Adrenal Vein Draining into the Renal Vein 2
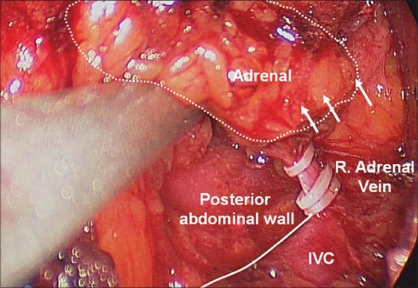
Right Adrenal Vein Draining into the IVC 2
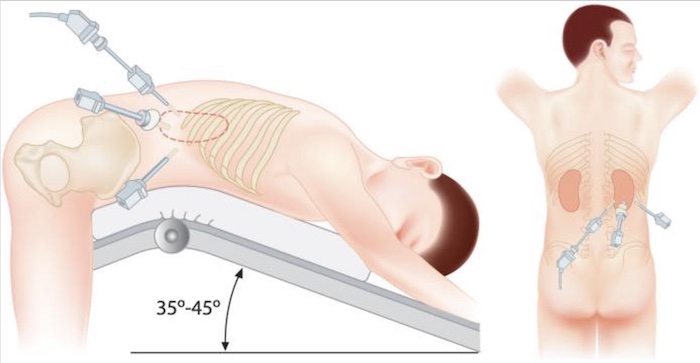
Retroperitoneoscopic Port Placement and Patient Positioning for Right Adrenalectomy 3
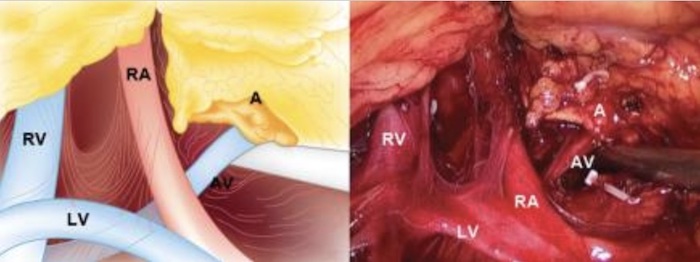
Left Retroperitoneoscopic View: Adrenal (A), Adrenal Vein (AV), Lumbar Vein (LV), Renal Vein (RV), and Renal Artery (RA) – Note Clips for the Inferior and Medial Adrenal Arteries 3
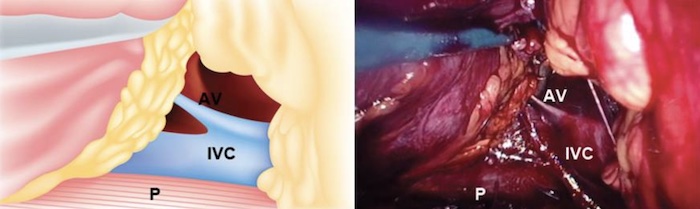
Right Retroperitoneoscopic View: Adrenal Vein (AV), IVC, and Psoas Muscle (P) 3