Vascular: Amputation
Amputation
Basics
- Largest Risk Factors: PAD & DM
- Should Generally Be Viewed as a Definitive Reconstructive Option, Not a Treatment Failure
Indications
- Acute Ischemia:
- Irreversible
- Severe with No Revascularization Options
- Failed Revascularization Attempts
- Chronic Ischemia:
- Failed Revascularization Attempts
- Severe with No Revascularization Options
- Severe Comorbidities
- Poor Functional Status
- Extensive Gangrene/Infection that is Not Salvageable
- Severe Infection Causing Pedal Sepsis
- Severe Traumatic Injury
- Malignancy
Amputation Staging
- Formal Amputation – Definitive Single-Stage Procedure
- Guillotine Amputation – Two-Stage Procedure
- First: Straight Amputation with Open Site
- Second: Formal Amputation a Few Days Later
Amputation Levels
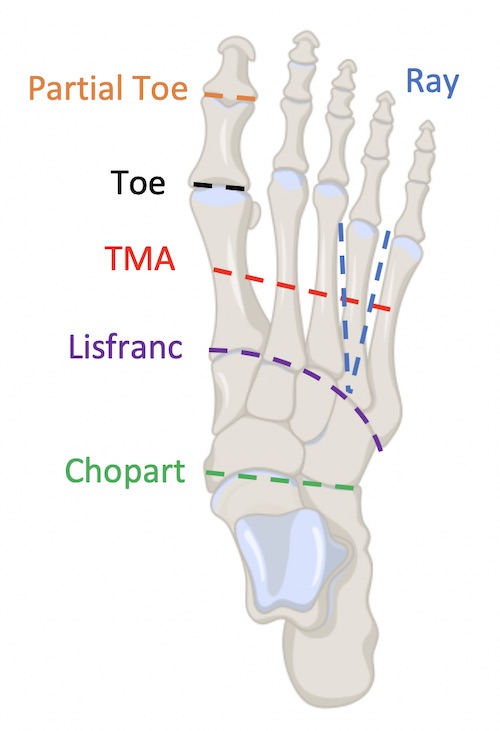
- Podiatric Procedures:
- Partial Toe Amputation – Part of a Toe
- Toe Amputation – Entire Toe
- Ray Amputation – Toe & Corresponding Metatarsal Bone
- Transmetatarsal Amputation (TMA) – Partial Foot Across the Metatarsal Bones
- Tarsometatarsal (Lisfranc) Amputation – Forefoot Amputation Across the Tarsometatarsal Line
- Midtarsal (Chopart) Amputation – Forefoot & Midfoot Amputation Sparing the Proximal Talus & Calcaneus
- Ankle Disarticulation (Syme’s Amputation) – Through Ankle Joint
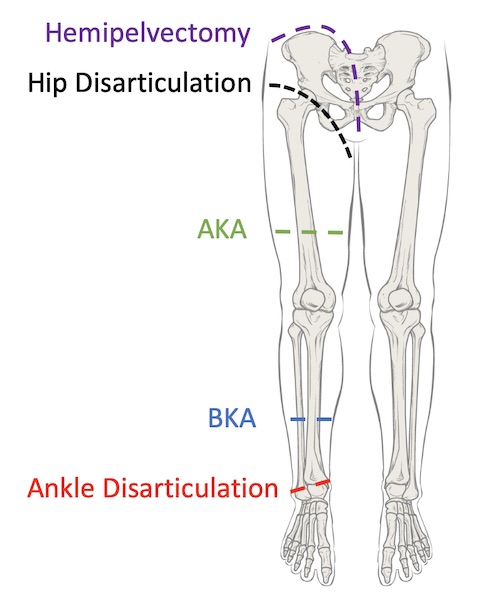
- Major Leg Amputations:
- Transtibial – Below-Knee Amputation (BKA)
- Transfemoral – Above-Knee Amputation (AKA)
- Orthopedic Hip Procedures:
- Hip Disarticulation – Entire Leg
- Hemipelvectomy – Entire Leg & Ipsilateral Hemipelvis
Testing to Determine Site
- Objective Data Can Supplement but Not Replace Clinical Judgment
- Transcutaneous Oxygen (tcPO2)
- Generally Considered the Best Objective Test
- Sensor Placed on Skin, Heated to Decrease Flow Resistance & Oxygen Partial Pressure Measured
- Approximates True Arterial Oxygen Pressure at Questioned Site
- Values:
- < 16-20 mmHg: Likely to Fail
- ≥ 20-30 mmHg: Likely to Heal
- Other Less Reliable Objective Tests
- Skin Temperature – Not Reliable
- Ankle Brachial Index (ABI)
- Arteriography – Poor Correlation to Healing Potential
Foot Amputations
Leg Amputations
Outcomes
- General Outcomes:
| Healing Rates | Mortality | |
| Overall | – | 8% |
| BKA | 80% | 5-7% |
| AKA | 90% | 10-15% |
| Hip Disarticulation | – | 50% |
- 10-20% of BKAs Require Revision to AKAs
- 10-20% Eventual Risk for Major Amputation on Contralateral Side
- Ambulation:
| Increased Energy Expenditure to Walk | Ambulation Rate | |
| BKA | 10-40% | 70-80% |
| AKA | 60-70% | 35-50% |
| Hip Disarticulation | 80% | 0-10% |
Complications
- Most Common Cause of Death: MI
- Contracture
- Risk: 3-5%
- Inhibits Proper Prosthetic Ambulation
- Prevention:
- BKA: Rigid Dressings
- AKA: Brief Periods of Prone Positioning
- Bleeding
- Risk of Reoperation for Bleeding Control: 4-8%
- Infection
- DVT
- Up to 50% Risk Without Prophylaxis
- Chronic Pain
- Phantom Pain – Poorly Understood
- Post-Traumatic Stress Disorder
- 5% Risk for Vascular Amputations
- 20% Risk for Traumatic Amputations
Transtibial – Below-Knee Amputation (BKA)
Posterior Flap Technique
- Skin/Fascia Incision:
- “Two-Thirds/One-Third” Approach
- Anterior Incision:
- Two-Thirds of Leg Circumference
- Start Just Past the Planned Tibia Incision
- Straight Transverse Incision
- Posterior Incision:
- One-Third of Leg Circumference
- Flap Length: Additional One-Third of Leg Circumference
- Slightly Curved Incision
- Bone Transection:
- Tibia: ≥ 12-15 cm Below Tibial Tuberosity
- Fibula: 1-2 cm Proximal to the Tibia
- Neurovascular Management:
- Major Blood Vessels: Suture Ligate
- Consider Tourniquet to Decrease Blood Loss
- Nerves: Divide Sharply & Allow Retraction
- Major Blood Vessels: Suture Ligate
- Modification & Closure:
- Bevel Bones to Avoid Sharp Edges – Particularly the Anterior Tibia
- Consider Myodesis of Gastrocnemius to Tibia
- Irrigate Prior to Closure
- Close Deep Fascia with Interrupted Absorbable Suture
- Close Skin with Staples
BKA Wound Dressing
- Soft Gauze with Elastic Wrap
- Most Commonly Used
- Remain Non-Weight Bearing for 4-6 Weeks Until Fit for Prosthesis
- Thigh-Level Rigid Plaster Cast
- Shorter Rehabilitation Times
- Similar Pain, Healing Rates & Prosthetic Use
- Can Include a Temporary Immediate Postoperative Prosthesis (IPOP)
- May Have Improved Primary Wound Healing & Shorter Rehabilitation Times

BKA Incision
Transfemoral – Above-Knee Amputation (AKA)
Fish-Mouth Technique
- Skin/Fascia Incision:
- “Fish-Mouth” Incision Made with Equal Anterior & Posterior Flaps
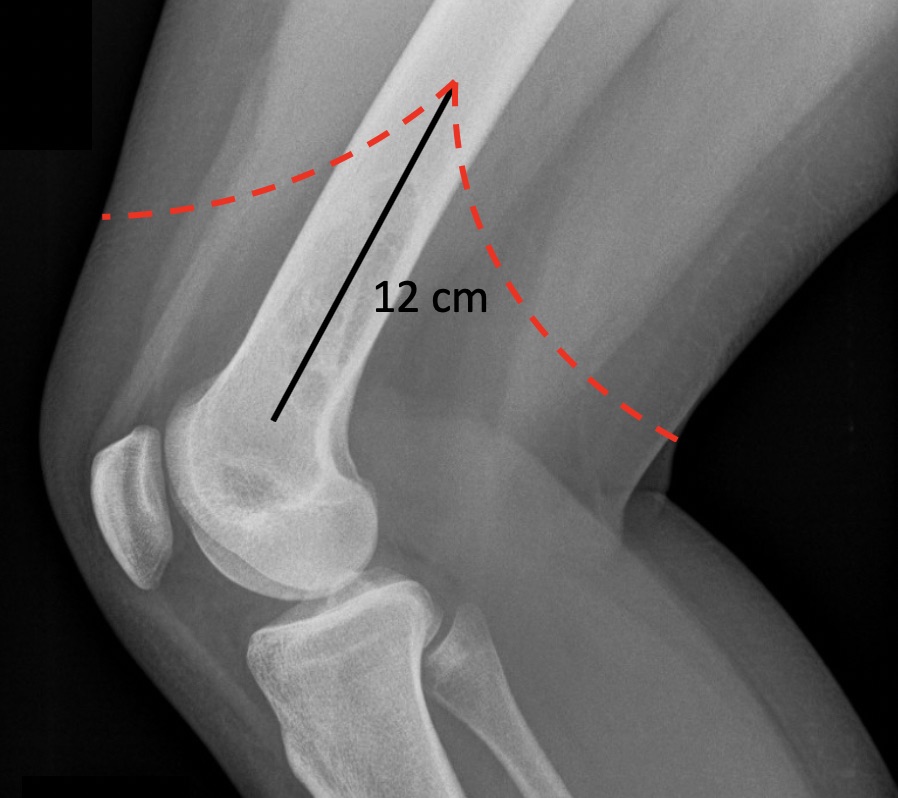
- Femur Transection: 12 cm Proximal to Femoral Condyles
- May Need to be More Proximal if Lacking Adequate Tissue Coverage
- Neurovascular Management:
- Major Blood Vessels: Suture Ligate
- Consider Tourniquet to Decrease Blood Loss
- Sciatic Nerve: Stretch & Divide Sharply, Then Allow Retraction
- Major Blood Vessels: Suture Ligate
- Modification & Closure:
- Bevel Bones to Avoid Sharp Edges – Particularly the Anterior Tibia
- Consider Myodesis of Adductor Magnus & Quadriceps Muscles
- Irrigate Prior to Closure
- Close Deep Fascia with Interrupted Absorbable Suture
- Close Skin with Staples
AKA Incision