Gupta MD, M P G, Mukhopadhyay S, Yusuf J, Tyagi S. Baller-gerold syndrome a rare cause of heart-hand syndrome. ISRN Cardiol. 2011;2011:962084. (License: CC BY-3.0)
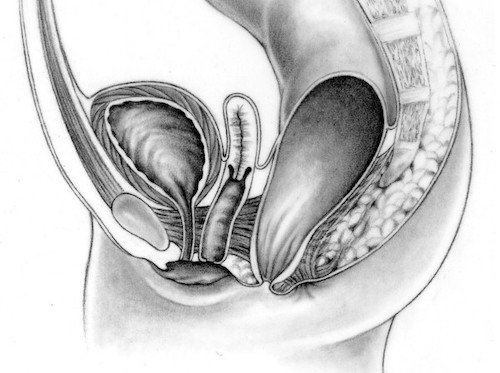
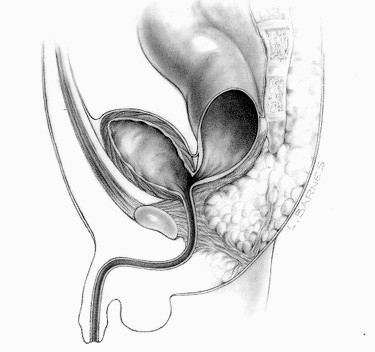
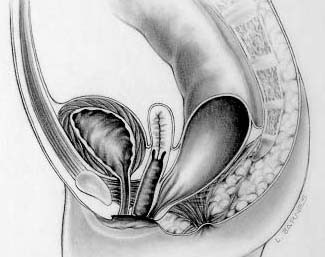
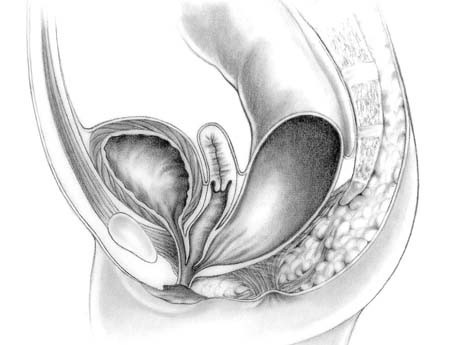
Levitt MA, Peña A. Anorectal malformations. Orphanet J Rare Dis. 2007 Jul 26;2:33. (License: CC BY-2.0)