Vascular: Abdominal Aortic Aneurysm (AAA)
Abdominal Aortic Aneurysm (AAA)
Basics
- Aneurysm Definition: 1.5x Dilation of Normal Vessel Diameter
- Normal Diameter: 2-3 cm
- Most Common Cause: Atherosclerosis with Degeneration of Media
- Most Common Site: Infrarenal (80%)
- Rupture Has a 40-50% Mortality
- Most Common Site: 2-4 cm Inferior to Renals; Left Posterolateral Wall
Risk Factors
- Disease Risk Factors:
- Smoking (Strongest Risk Factor)
- Male
- Elderly
- Hypertension
- White
- Spinal Cord Injury
- Rupture Risk Factors:
- Hypertension
- COPD
- Overall Size
- Rapid Increase in Size
- Female Sex
Presentation
- Mostly Asymptomatic & Found Incidentally
- Rupture Triad:
- Acute Abdominal or Back Pain
- Hypotension
- Pulsatile Abdominal Mass
Diagnosis
- Screening: Duplex US
- One-Time US Indications:
- Age 65 with Tobacco History (Smoked ≥ 100 Cigarettes)
- Age 65 with First-Degree Relatives with AAA’s
- Surveillance Frequency (SVS Guidelines):
- ≥ 3.0 cm: Every 3 Years
- ≥ 4.0 cm: Every 12 Months
- ≥ 5.0 cm: Every 6 Months
- US is Good for AAA But Poor at Identifying Rupture
- One-Time US Indications:
- Surgery Planning: CTA
- Ruptured:
- Stable, Transient Responder or Insufficient Evidence: CTA
- Unstable & Sufficient Clinical Evidence: Proceed Directly to Surgery
Repair Indications
- Symptomatic
- Large
- Males ≥ 5.5 cm
- ≥ 5.0 cm if High Rupture Risk (COPD, Poorly Controlled HTN)
- Females ≥ 5.0 cm
- Males ≥ 5.5 cm
- Growth > 1 cm Per Year
- Peripheral Ischemia from Embolization of Mural Thrombosis
- Mycotic Aneurysm
Repair
- Stable: Elective Open Repair or Endovascular Aneurysm Repair (EVAR)
- EVAR Often Preferred (Especially if High Risk, Elderly or Multiple Comorbidities)
- EVAR Requirements/Contraindications:
- Comparison:
- Similar Mortality if Ruptured
- Short-Term (30-Day) Mortality:
- EVAR – 2-4% (Better)
- Open – 5-7%
- Similar Long-Term Mortality
- Unstable: Emergent Open Repair or Endovascular Aneurysm Repair (EVAR)
- Allow Permissive Hypotension: SBP 50-100
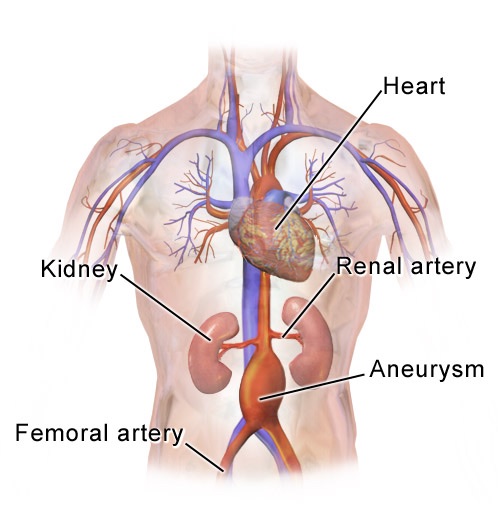
AAA 1
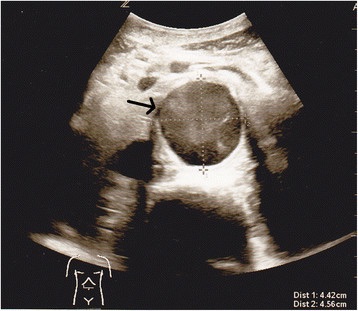
AAA by Duplex US 2
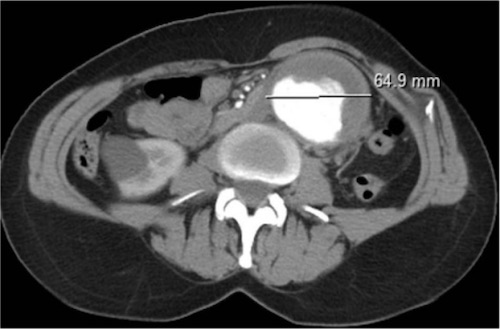
AAA by CTA 3
Other Aortic Aneurysms
Inflammatory Aneurysm
- Aneurysmal Dilation Due to Significant Inflammation
- Thick Aortic Wall with Adjacent Retroperitoneal Fibrosis
- Dense Adherence to Adjacent Structures
- Etiology Not Entirely Understood
- Specific Issues:
- Adhesions to Duodenum & Small Bowel
- Ureter Entrapment
- Tx: Stent Grafting (Inflammation Resolves with Graft)
Mycotic Aneurysm
- Infected Aneurysm
- Most Common Organisms: Staphylococcus #1, Salmonella #2, Escherichia coli & Streptococcus
- Most Common Non-Aneurysmal Infection: Salmonella
- More Often Saccular than Fusiform
- High Risk of Rupture
- CT Findings:
- Periaortic Soft Tissue Mass
- Fluid Stranding
- Destruction of Surrounding Tissues
- Tx: ABX & Surgical Repair (Reconstruction or Extra-Anatomic Bypass)
References
- Blaus B. Wikimedia Commons. (License: CC BY-SA-4.0)
- Spangler R, Van Pham T, Khoujah D, Martinez JP. Abdominal emergencies in the geriatric patient. Int J Emerg Med. 2014 Oct 21;7:43.(License: CC BY-4.0)
- Jiber H, Hajji R, Zrihni Y, Zaghloul R, Zizi O, Bouarhroum A. Isolated infrarenal abdominal aorta aneurysm in a 42-year-old patient with Marfan’s syndrome: Case report. SAGE Open Med Case Rep. 2013 Oct 1;1:2050313X13507564. (License: CC BY-NC-3.0)