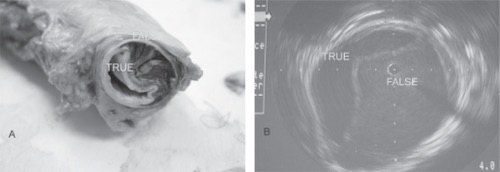
Aortic Dissection Specimen and Intravascular Imaging 1
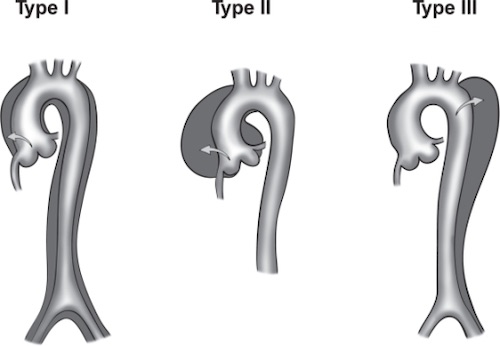
DeBakey Classification 1
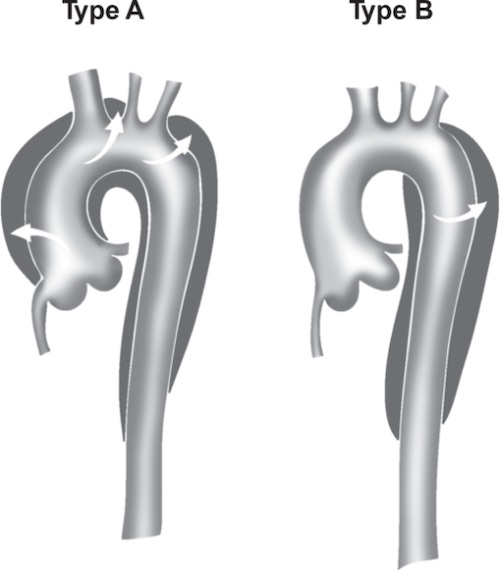
Stanford Classification 1
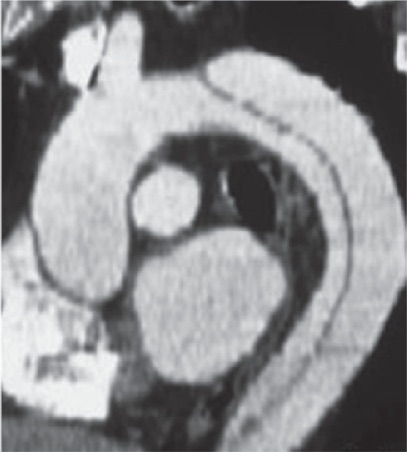
Aortic Dissection on CTA 1
Aortic Dissection Specimen and Intravascular Imaging 1
DeBakey Classification 1
Stanford Classification 1
Aortic Dissection on CTA 1