
Breast Examination 1
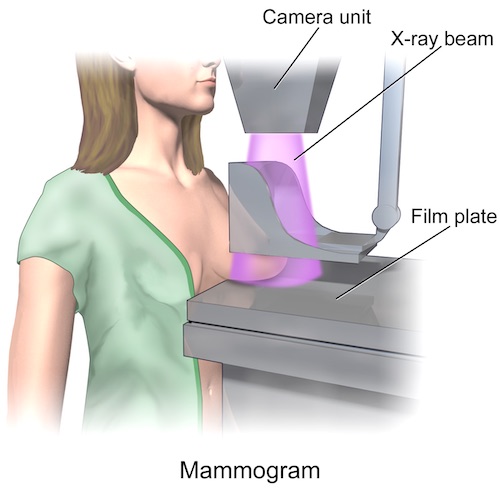
Mammogram 2

Normal Mammogram 3
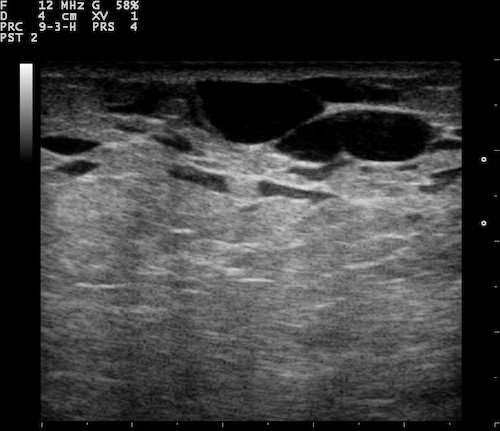
Normal Breast Ultrasound; Showing Ducts 4
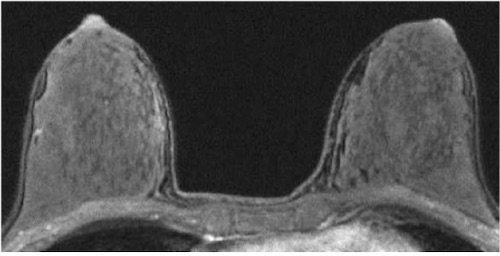
Breast MRI 5

Core Needle Biopsy 6
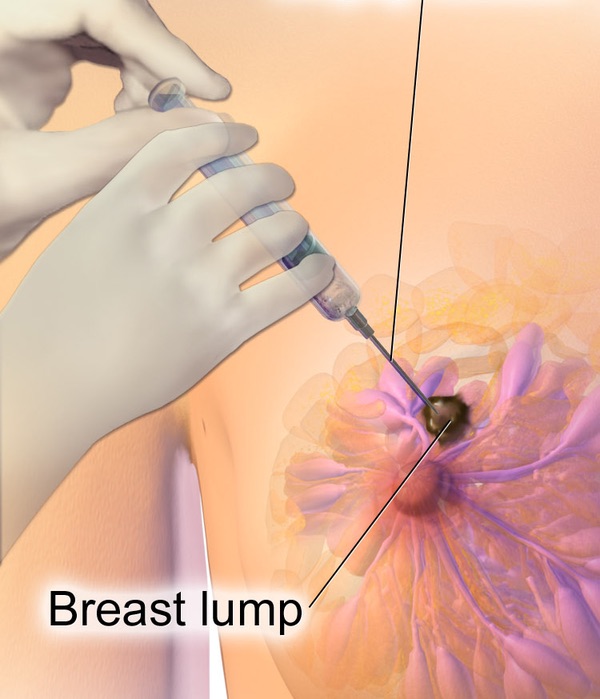
Breast FNA 7
Breast Examination 1
Mammogram 2
Normal Mammogram 3
Normal Breast Ultrasound; Showing Ducts 4
Breast MRI 5
Core Needle Biopsy 6
Breast FNA 7