Small Intestine: Carcinoid Tumor
Carcinoid Tumor
Pathophysiology
- Well-Differentiated Neuroendocrine Tumor Arising from Gastrointestinal Enterochromaffin (Kulchitsky) Cells
- Produce:
- Serotonin (Metabolized to 5-HIAA)
- Kallikrein
- Histamine
- Tachykinins
- Prostaglandin
Location
- Most Common Site: Small Intestine (50%) < Rectum < Appendix < Colon < Stomach
- Most Common in Ileum
- *Past Believed That the Appendix Was Most Common
- Most Common Primary Small Intestine Tumor
- Gastric Tumor Types (If in Stomach)
- Type I: Associated with Chronic Atrophic Gastritis & Pernicious Anemia
- Most Common Gastric Subtype (70-80%)
- Grow Slowly
- Type II: Associated with Gastrinoma & Possibly MEN-I
- Intermediate Growth
- Type III: Sporadic
- Aggressive
- Type I: Associated with Chronic Atrophic Gastritis & Pernicious Anemia
Presentation
- Most Common Presenting Sx: Abdominal Pain
- Carcinoid Syndrome
- Infrequently Encountered
- Occurs Once Tumor Metastasizes to Liver or Retroperitoneum
- Serotonin Cleared in Liver & Lung by Monoamine Oxidase if Only Produced by GI Tract
- Sx:
- Flushing (From Kallikrein)
- Clinical Hallmark of Carcinoid Syndrome (85%)
- Diarrhea (From Serotonin)
- Bronchoconstriction (From Bradykinin)
- Right Heart Valve Lesions & Tricuspid Insufficiency
- Venous Telangiectasia (From Prolonged Vasodilation of Face)
- Flushing (From Kallikrein)
- Carcinoid Crisis
- The Release of an Overwhelming Amount of Hormone from the Tumor
- Causes Hemodynamic Instability & Symptoms of Carcinoid Syndrome
- Triggers:
- Anesthesia Induction
- Tumor Manipulation (Biopsy or Manual Palpation)
- Invasive Procedures
- Less Common:
- Chemotherapy
- Hepatic Artery Embolization
Prognosis
- 25% Have More Than One Small Bowel Tumor at Diagnosis
- 40-80% Have Spread to the Mesentery with Nodal Metastases at Diagnosis
- 2/3 Have Spread by Time of Dx (Local or Systemic)
Diagnosis
- CT of Mesenteric Masses Classically Show a Spiculated Mass with Calcification & Desmoplastic Reaction
- Detect:
- Urinary 5-HIAA
- Best Initial Test
- Low Sensitivity if Non-Functioning
- Chromogranin A Level
- Can Also Detect Non-Functioning
- Low Specificity (Not for Diagnosis)
- Use: Progression, Response & Recurrence
- Urinary 5-HIAA
- Localize:
- Octreotide Scan
- 68 Ga-DOTATATE PET/CT Scan – Generally Preferred if Available
- Superior Image Quality with Greater Patient Convenience (Octreotide Scan May Require Repeat Images the Next Day)
Treatment
- Primary Tx: Resection
- If Unresectable: Chemo (Streptozocin & 5FU) & Octreotide
- Liver Mets: Resect if Able
- Contraindications:
- Diffuse Bilobar Involvement
- Compromised Liver Function
- Extrahepatic Metastases
- Presence of Poorly-Differentiated Carcinoma
- Consider Preoperative Hepatic Artery Embolization
- Very Good Survival Rates Even with Extensive Liver Mets
- Contraindications:
- Symptomatic Tx:
- Flushing: α-Blockers
- Other Symptoms: Octreotide
- Carcinoid Crisis: Octreotide
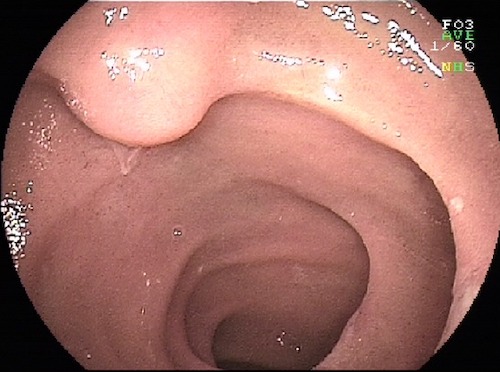
Carcinoid Tumor in Ileum 1

Carcinoid Tumor in Jejunum 2
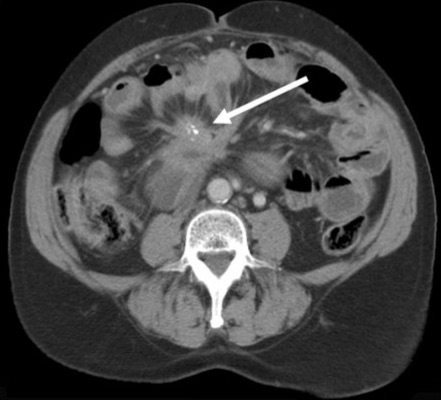
Carcinoid Tumor with Calcified Mesenteric Mass 3
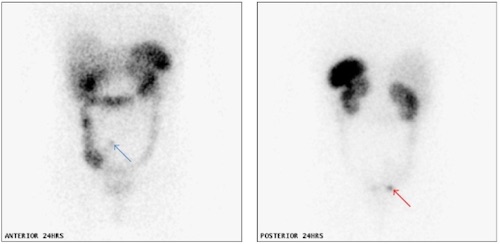
Carcinoid Tumor on Octreotide Scan 4
Carcinoid Tumor – Extent of Resection
Stomach
- Type I/II:
- < 1-2 cm: Endoscopic Resection
- > 2 cm: Surgical Resection
- Consider Antrectomy if Type I with Numerous Progressive Tumors
- Type III: Gastrectomy (Partial vs. Total)
Small Bowel
- Most: En Bloc Resection with Wide Lymphatic Mesenteric Clearance
- *Some Consider Segmental Resection Alone if Single & < 1 cm with No Nodal Mets
- Periampullary: Pancreaticoduodenectomy
- Terminal Ileum: Right Hemicolectomy
Appendix
- Tip & < 2 cm: Appendectomy
- Base or ≥ 2cm: Right Hemicolectomy
- Other Indications: Positive LN, Grade II or Mixed Histology (Goblet Cell)
Colon
- < 1 cm: Endoscopic Polypectomy
- > 1 cm: Partial Colectomy & Regional Lymphadenectomy
Rectum
- High Rectum
- < 1 cm: Endoscopic Polypectomy
- 1-2 cm: Debated (Polypectomy vs Resection)
- > 2 cm: Resection (LAR/APR)
- Low Rectum
- < 2 cm: WLE
- > 2 cm: Resection (APR)
- Or If Invades Muscularis Propria
References
- Kopáčová M, Rejchrt S, Bureš J, Tachecí I. Small intestinal tumours. Gastroenterol Res Pract. 2013;2013:702536. (License: CC BY-3.0)
- Pillay Y. An intestinal carcinoid causing transient jejunal intussusception in an adult-A case report. Int J Surg Case Rep. 2017;31:20-23. (License: CC BY-NC-ND-4.0)
- Patel CM, Sahdev A, Reznek RH. CT, MRI and PET imaging in peritoneal malignancy. Cancer Imaging. 2011 Aug 24;11(1):123-39. (License: CC BY-4.0)
- Sewpaul A, Bargiela D, James A, Johnson SJ, French JJ. Spontaneous Regression of a Carcinoid Tumor following Pregnancy. Case Rep Endocrinol. 2014;2014:481823. (License: CC BY-3.0)