Type III (“Cecal Bascule”): Anterosuperior Folding of the Cecum without Any Axial Twisting
Less Common (20%)
Cecal Volvulus 1
Etiology
Congenital Risk Factors
Mobile Cecum and Ascending Colon (Congenital Failure of Normal Peritoneal Fixation During Development)
Malrotation or Incomplete Intestinal Rotation
Congenital Bands or Adhesions
More Common in the 4th-6th Decade of Life (Compared to Sigmoid Volvulus Which is Most Common in the 6th-8th Decade of Life) – Due to Congenital Cecal Mobility Rather than Degenerative Colonic Disease
Additional Risk Factors
Adhesions
Female Sex
Pregnancy
Chronic Constipation
Colonic Dysmotility
High-Fiber Intake
Abdominal Masses
Prolonged Immobility
Colonoscopy
Presentation and Diagnosis
Presentation
Abdominal Pain
Abdominal Distention
Nausea and Vomiting
Obstipation
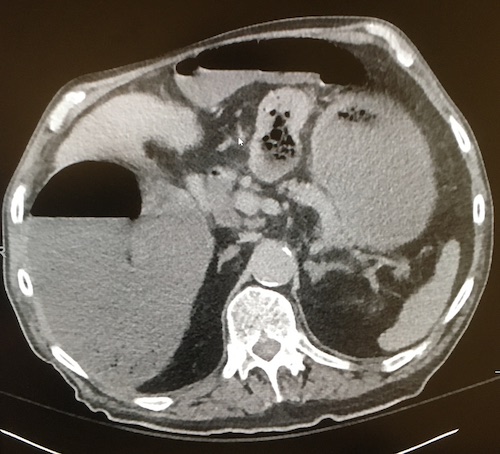
Diagnosis
Generally Diagnosed by CT Abdomen/Pelvis
Cecum is Dilated and Twisted
Ileocecal Valve May Be Directed Laterally
“Whirl Sign” with Mesentery Twisted
Abdominal Plain Film Can Be Diagnostic But is Neither Sensitive nor Specific
Classic “Coffee-Bean Sign” (Dilated Loop of Colon with Apex in the Left Upper Quadrant) is Rarely Seen
Suggestive Plain Film Findings Should Be Further Evaluated by CT
Can Be Diagnosed at Surgical Exploration in an Emergent Setting
Cecal Bascule
Management
The Primary Treatment is Surgical Resection (Right Hemicolectomy vs Ileocecectomy)
Avoid Endoscopic Detorsion – Technically Difficult with High Risk for Perforation and Missed Injury
Surgical Intervention
Do Not Detorse Ischemic or Necrotic Bowel Prior to Resection – Risk for Reperfusion Bacteremia and Sepsis
Detorsion Alone without Resection is Generally Advised Against Due to High Recurrence Rate (Up to 25% or More)
Consider End Ileostomy vs Anastomosis with Diverting Loop Ileostomy if High Risk for Anastomotic Leak
May Consider Detorsion and Cecopexy Alone (Without Resection) if Bowel is Viable and the Patient is Hemodynamically Unstable or Unfit for Resection
Alternatively May Consider Detorsion with Cecostomy Tube Instead of Cecopexy
References
James B, Kelly B. The abdominal radiograph. Ulster Med J. 2013 Sep;82(3):179-87. (License: CC BY-NC-SA-4.0)