Trauma: Chest Wall Trauma
Chest Wall Injury
AAST Chest Wall Injury Scale
- *See AAST
- Injury Scale is Under Copyright
Rib Fracture
Respiratory Splinting
- Definition: Reduced Inspiratory Effort Due to Severe Pleuritic Chest Pain Upon Inspiration
- Results In:
- Hypoventilation
- Atelectasis
- Pneumonia
- Retained Secretions
- Respiratory Failure
- Can Quantify with Incentive Spirometry (IS)
- Goal: > 15 cc/kg Ideal Body Weight
Elderly
- Most Common Injury in Elderly After Blunt Chest Trauma
- Each Additional Rib Fracture Increases:
- Risk of Death by 19%
- Risk of PNA by 27%
- *Risk May Be Overestimated by Older Studies without Modern Imaging
Descriptions
- Types:
- Simple: Single Fracture Line Across the Rib with No Fragmentation or Comminution
- Wedge: A Second Fracture Line that Does Not Span the Entire Rib Width
- Complex: ≥ 2 Fracture Lines with ≥ 1 Fragment Spanning the Entire Rib Width
- Displacement:
- Nondisplaced: ≥ 90% of the Fracture Cortical Surfaces are in Contact
- Offset: Some Cortical Contact But < 90% of the Fracture Cortical Surfaces are in Contact
- Displaced: No Cortical Contact Between Fracture Surfaces
- Location:
- Anterior: Anterior to the Anterior Axillary Line
- Lateral: Between the Anterior & Posterior Axillary Lines
- Posterior: Posterior to the Posterior Axillary Line
Diagnosis
- May Be Seen on CXR but Often Underestimates or Misses
- CXR Sensitivity Only 33-40%
- CT is the Gold Standard – Also Able to Provide 3D Reconstructions for Surgical Planning
Flail Chest
- Definitions:
- Flail Segment: ≥ 3 Adjacent Ribs Fractured in ≥ 2 Places
- *Some Texts Say ≥ 2 Adjacent Ribs Fractured in ≥ 2 Places
- Flail Chest: Flail Segment with the Clinical Paradoxical Chest Wall Movement
- Flail Segment: ≥ 3 Adjacent Ribs Fractured in ≥ 2 Places
- Paradoxic Breathing – Segment Pulled Inward with Inhalation & Outward with Exhalation
- Disrupts Normal Respiratory Mechanics
- Collapse Causes Air Movement from the Injured Lung to the Uninjured Lung – Results in a Possible Mediastinal Shift to the Injured Side
- Risk for Underlying Pulmonary Contusion
- Initial CXR Underestimates & Worsens with Time and IVF Resuscitation
Treatment
- Primary Tx: Aggressive Pain Control & Pulmonary Therapy
- Consider Epidural Analgesia as the Primary Pain Control Modality for Severe Blunt Thoracic Trauma with Multiple Rib Fractures
- In Elderly Patients: Consider Admission to ICU (High Mortality Risk)
- Rib Plating (ORIF) Indications:
- Significant Flail Segment if No Underlying Contusion
- Nonunion
- Significant Deformity
- Refractory Pain
- Unable to Wean Off Ventilator
- During Thoracotomy for Other Indication – “On the Way Out”
- *Exact Indications are Debated & Evolving
- Typical Ribs Plated:
- Ribs #1-3: Not Plated
- Have Little Movement & Are Difficult to Access
- Ribs #4-9: The Only Ribs Plated
- Where the Majority of Chest Wall Movement Occurs
- Ribs #10-12: Not Plated
- Add Little to Chest Wall Stability
- Ribs #1-3: Not Plated
Pain Control Options
- Multimodal Approach:
- Ice Packs/Heat Packs
- Acetaminophen
- Ibuprofen
- Gabapentin
- Muscle Relaxants (Flexeril)
- Lidocaine Patches
- Ketamine
- PO Narcotics
- IV Narcotics/PCA
- Nerve Block
- Erector Spinae Block
- Epidural Analgesia

Flail Chest 1
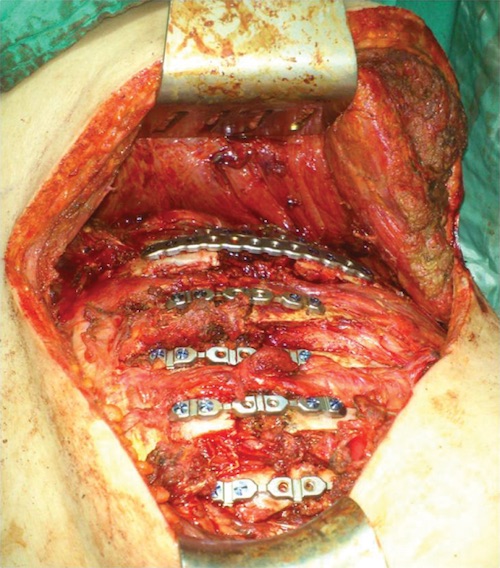
Rib Plating 2
Sternal Fracture
General
- Significant Force Required to Fracture, Often Multiple Injuries Present
- No Increased Concern for Underlying Cardiac Contusion
- *Previously Believed to Be
Most Common Associated Injuries
- Rib Fracture (57.8%) – Most Common
- Lung Contusion (33.7%)
- Pneumothorax (22.0%)
- Vertebral Fracture (21.6%)
- Lumbar Vertebrae Fracture (16.9%)
- Concussion (3.9%)
- Blunt Cardiac Injury (3.6%)
Diagnosis
- Dx: CT
- CXR Only 50% Sensitive
Treatment
- Tx: Supportive
- ORIF Indications: Chronic Pain or Unstable

Sternum Fracture 3
Scapula Fracture
General
- Significant Force Required to Fracture, Often Multiple Injuries Present
- Dx: CXR/CT
Treatment
- Tx: Supportive (Sling for 2 Weeks)
- ORIF Indications:
- Open Fracture
- Glenoid Instability
- Loss of Rotator Cuff Function
- Unstable Neck Fractures
- Significant Displacement
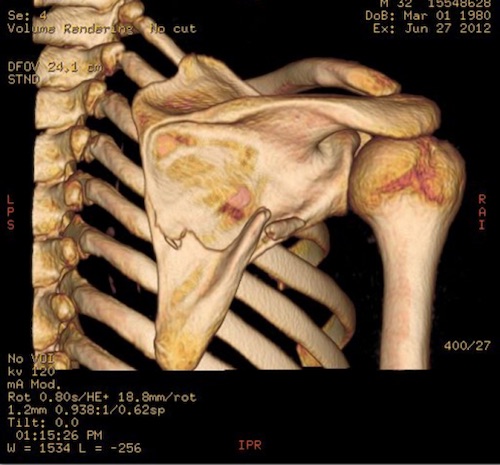
Scapula Fracture 4
Clavicle Fracture
General
- Often Occur in Isolation (Opposed to Sternum/Scapula Fractures)
- Mostly from Falling on An Outstretched Arm or Direct Blow
Allman Classification
- Group I: Middle Third (69-80%) – Most Common Site
- Group II: Distal Third (10-28%)
- Group III: Proximal Third (2-9%)
Treatment
- Tx: Conservative
- Sling with ROM Exercises vs Figure-of-Eight Bandage
- Surgery (ORIF or Intramedullary Fixation) Indications:
- Open Fractures
- Displaced with Skin Tenting
- Associated Neurovascular Injury
- Floating Shoulder (Scapula Neck & Clavicle Fracture)
- Nonunion with Refractory Pain

Clavicle Fracture
Extrapleural Hematoma
General
- Hematoma of the Extrapleural Space
- Often Confused with HTX
Types
- Nonconvex: Smaller, Likely Due to Venous Injury
- Biconvex: Larger, Likely Due to Arterial Injury
- More Likely to Require Surgical Intervention
Diagnosis
- Sx: Bleeding, Chest Pain & Shortness of Breath
- Most ASx
- Dx: CT
- “Extrapleural Fat Sign” – Inward Displacement of Extrapleural Fat
Treatment
- Small/Stable: Conservative Management
- Large/Cardiorespiratory Sx: VATS
- If Fails: Thoracotomy

Extrapleural Hematoma
References
- Granhed HP, Pazooki D. A feasibility study of 60 consecutive patients operated for unstable thoracic cage. J Trauma Manag Outcomes. 2014 Dec 30;8(1):20. (License: CC BY-2.0)
- Evman S, Kolbas I, Dogruyol T, Tezel C. A Case of Traumatic Flail Chest Requiring Stabilization with Surgical Reconstruction. Thorac Cardiovasc Surg Rep. 2015 Dec;4(1):8-10. (License: CC BY-NC-SA-4.0)
- Lahham S, Patane J, Lane N. Ultrasound of Sternal Fracture. West J Emerg Med. 2015 Dec;16(7):1057-8. (License: CC BY-4.0)
- Memişoğlu S, Yılmaz B, Aktaş E, Kömür B. Isolated scapula fracture: Ice hockey player without trauma. Ann Med Surg (Lond). 2015 Jul 29;4(3):235-7. (License: CC BY-NC-ND-4.0)