If Imaging Indeterminate: Tissue Dx (FNA/Brush Cytology/IR Bx)
Tumor Markers:
CA 19-9 – Elevated
CEA – Elevated
AFP – Normal (Differentiate From HCC)
Treatment
Unresectable Features:
Extrahepatic Organ Invasion
LN Beyond Hepatoduodenal Ligament (Periaortic or Celiac)
Mets or Disseminated Disease
Invades Main Portal Vein or Hepatic Artery (Some Centers May Reconstruct)
Resectable Tx:
Surgery:
Distal CBD: Pancreaticoduodenectomy
Compared to Whipple for Pancreatic Adenocarcinoma
Higher Survival
Higher Incidence of Postoperative Pancreatic Fistula
Perihilar: En Bloc Resection (Extrahepatic Bile Ducts/Gallbladder) & Roux-en-Y Hepaticojejunostomy
Type III/IV: Add Hepatic Lobectomy
Intrahepatic: Hepatic Resection
Consider Preoperative Biliary Drainage if Have Obstructive Jaundice (Controversial)
Adjuvants:
Neoadjuvant Chemo – Only for Highly-Selected Patients
Adjuvant Chemo – Indicated for All Resectable Patients
Also Consider XRT
Liver TXP – Possibly in Setting of PSC or if Small but Unresectable
Used for Hilar Tumors but Not if Intrahepatic
Unresectable Tx:
Unresectable/Mets: Chemotherapy
Obstruction Palliation: Stents
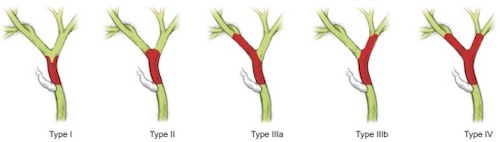
Bismuth-Corlette Classification of Cholangiocarcinoma 2
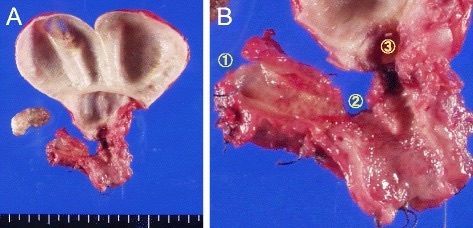
MRI of Intrahepatic Cholangiocarcinoma 3
Cholangiocarcinoma: TNM Staging – AJCC 8
Distal CBD Cholangiocarcinoma
TNM
T
N
M
1
Depth < 5 mm
1-3
Mets
2
Depth 5-12 mm
≥ 4
3
Depth > 12 mm
4
Invades Celiac Axis, SMA or Hepatic Artery
Stage
T
N
M
I
T1
N0
M0
II
A
T1
N1
M0
T2
N0
M0
B
T2
N1
M0
T3
N0-1
M0
III
A
T1-3
N2
M0
B
T4
Any N
M0
IV
Any T
Any N
M1
Perihilar Cholangiocarcinoma
TNM
T
N
M
1
Confined to Duct
1-3 LN
Mets
2
A – Invades Adipose Tissue
B – Invades Liver
≥ 4 LN
3
Invades Branch of Portal Vein or Hepatic Artery
4
Invades Portal Vein or Hepatic Artery
Stage
T
N
M
I
T1
N0
M0
II
T2
N0
M0
III
A
T3
N0
M0
B
T4
N0
M0
C
Any T
N1
M0
IV
A
Any T
N2
M0
B
Any T
Any N
M1
Intrahepatic Cholangiocarcinoma
TNM
T
N
M
1
Solitary without Vascular Invasion
A – ≤ 5 cm
B – > 5cm
Any LN
Mets
2
Multiple or Invades Vasculature
3
Perforates Visceral Peritoneum
4
Invades Extrahepatic Structures
Stage
T
N
M
I
A
T1a
N0
M0
B
T1b
N0
M0
II
T2
N0
M0
III
A
T3
N0
M0
B
T4
N0
M0
Any T
N1
M0
IV
Any T
Any N
M1
Mnemonics
Bismuth-Corlette Classification of Cholangiocarcinoma
Type I: “I” – Main Trunk (CBD or Common Hepatic Duct)
Type II: “2 – Bi” – At the Bifurcation
Type III: “I/I” – One or the Other Unilateral Hepatic Ducts
Type IV: “Four Gets More” – Bilateral Hepatic Ducts
References
Okabe H, Chikamoto A, Maruno M, Hashimoto D, Imai K, Taki K, Arima K, Ishiko T, Uchiyama H, Ikegami T, Harimoto N, Itoh S, Yoshizumi T, Beppu T, Baba H, Maehara Y. A long survivor with local relapse of hilar cholangiocarcinoma after R1 surgery treated with chemoradiotherapy: a case report and literature review. Surg Case Rep. 2016 Dec;2(1):69. (License: CC BY-4.0)
Blechacz B. Cholangiocarcinoma: Current Knowledge and New Developments. Gut Liver. 2017 Jan 15;11(1):13-26. (License: CC BY-NC-4.0)
Jeong WK, Kim YK, Song KD, Choi D, Lim HK. The MR imaging diagnosis of liver diseases using gadoxetic acid: emphasis on hepatobiliary phase. Clin Mol Hepatol. 2013 Dec;19(4):360-6. (License: CC BY-NC-3.0)