Common Bile Duct Exploration (CBDE)
David Ray Velez, MD
The Operative Review of Surgery. 2023; 1:41-47.
Table of Contents
Laparoscopic Common Bile Duct Exploration
Definition
- Laparoscopic Exploration of the Common Bile Duct to Remove Stones
- *See Choledocholithiasis
Approaches
- Transcystic Approach – Through the Cystic Duct
- Preferred Approach if Able – Protect Integrity of the Common Bile Duct
- Choledochotomy – Through the Common Bile Duct
- Indicated if Transcystic Approach Fails or is Contraindicated
Comparison to Preoperative ERCP 1,2
- Lap-CBDE Has Lower Risk of Technical Failure
- Lap-CBDE Has Lower Risk of Overall Complications
- Lap-CBDE Has Lower Risk of Pancreatitis or Perforation
- Lap-CBDE Has Higher Risk of Bile Leak
- Lap-CBDE Has Shorter Length of Stay
- Lap-CBDE Has Fewer Procedures Required
Indications 4
- Choledocholithiasis Diagnosed Preoperatively by MRCP or US
- Choledocholithiasis Diagnosed Intraoperatively by Cholangiography
- Choledocholithiasis After Failed ERCP
- Choledocholithiasis with Altered Anatomy Unable to Undergo Traditional ERCP (Gastric Bypass, etc.)
Contraindications 4-6
- Hemodynamic Instability
- Hostile Porta Hepatis
- Contraindications to a Transcystic Approach:
- Friable Cystic Duct
- Narrow or Tortuous Cystic Duct
- Large Stones (> 1 cm)
- Multiple Stones (> 8-10)
- Common Hepatic Duct Stones
- Contraindications to a Choledochotomy:
- Narrow Common Bile Duct (Diameter < 7 mm)
Transcystic Procedure
- Generally Attempt Stone Clearance by IOC with Glucagon/Flushing First
- Proceed if Flushing Fails
- *See Intraoperative Cholangiogram (IOC)
- Dilate the Cystic Duct to 4-6 mm for Instrumentation
- Maximum 8 mm if Needed
- Retrieve Stones with Instrumentation Through the Cystic Duct Opening
- *See Below
- Confirm Clearance with a Completion Cholangiography
- Close the Ductal Stump
- Close Using an Endoloop (Not Clips) to Minimize the Chance of Leak Due to Edema
Choledochotomy Procedure
- Choledochotomy Incision
- 0-1.5 cm Longitudinal Incision Below the Cystic Duct Insertion
- Slightly Medial to Anterior Midline (Avoid Septum of Fused Cystic/CHD)
- Consider Stay Sutures on Either Side to Keep Open
- Retrieve Stones with Instrumentation Through the Common Bile Duct – Same Methods as Transcystic Approach
- *See Below
- Close Choledochotomy
- Classically Use an Absorbable Monofilament Suture
- May Consider Using an Absorbable Knotless Unidirectional Barbed Suture – Facilitates Easier Intracorporal Closure without Increased Complications 8-10
- May Consider Closing Over a T-Tube Although Falling Out of Favor 11,12
Options If Stone is Impacted and Unable to Remove Laparoscopically
- Conversion to an Open Common Bile Duct Exploration
- Leave T-Tube
- Postoperative ERCP
- If Preoperative ERCP Failed:
- Transduodenal Sphincteroplasty
- Biliary-Enteric Drainage (Side-to-Side Choledochoduodenostomy)
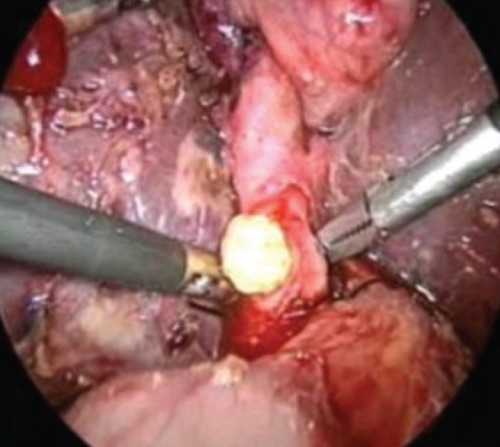
Laparoscopic Stone Removal by Choledochotomy 7
Stone Retrieval Techniques
Fogarty/Balloon Catheter
- Use a 4-Fr or 5-Fr Fogarty Catheter
- Balloon Catheter Fed Past the Stone into the Duodenum
- Balloon Inflated and Slowly Retracted Pulling the Stone Retrograde
- Stone Pulled Out Through the Ductal Opening
Balloon Sphincteroplasty
- Use a Balloon Catheter Under Fluoroscopic Guidance to Dilate the Sphincter of Oddi
- First Gain Guidewire Access into the Duodenum
- Advance a Balloon Catheter Over the Guidewire into the Duodenum
- Inflate Balloon in the Duodenum and Retract Under Fluoroscopic Guidance
- Determine Location of the Sphincter
- Slightly Deflate, Retract Balloon into the Sphincter, then Reinflate for 3-5 Minutes
- Larger Balloon Sizes (≥ 10 mm) Prevent Pancreatitis – Limits Postoperative Sphincter Spasm
- Balloon Should Not Be Larger than the Pathologically Dilated Bile Duct
- Can Then Facilitate Antegrade Stone Clearance – Done by Flushing, Pushing with a Choledochoscope, or Pushing with a Balloon Catheter Over a Guidewire
Choledochoscope-Guided Wire Basket
- Choledochoscope Insert Through the Ductal Opening
- May Use Ureteroscope if Dedicated Choledochoscope is Unavailable
- Continuous Saline Infusion to Dilate the Lumen & Permit Visualization
- Wire Basket Passed Beyond the Stone & Opened
- Ensnare Stone by Retracting Basket with Rotation
- Stone Pulled Out Through the Ductal Opening
Fluoroscopic-Guided Wire Basket
- Performed Under Fluoroscopic Guidance
- Guidewire Passed into the Duodenum Through the Ductal Opening
- Wire Basket Fed Over the Guidewire
- Ensnare Stone by Retracting Basket with Rotation
- Stone Pulled Out Through the Ductal Opening
Novel Approaches
- Lithotripsy
- Antegrade Sphincterotomy – Sphincterotome Inserted Through the Cystic Duct to Create a Sphincterotomy
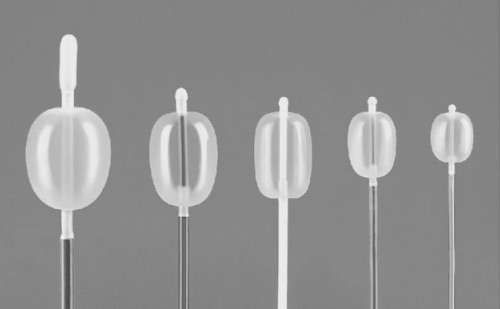
Fogarty Balloon Catheters 13
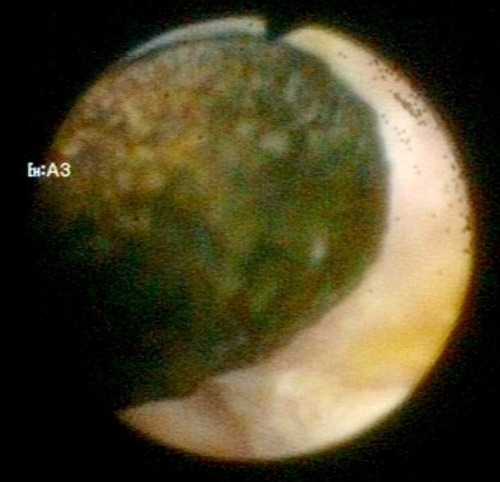
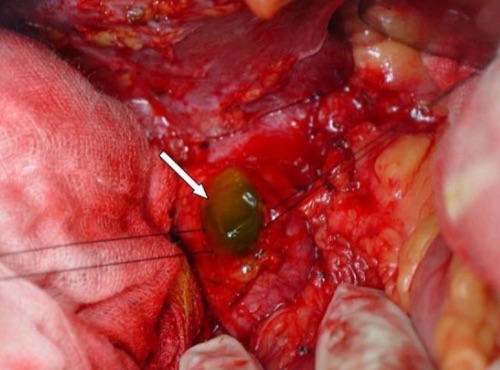
Large CBD Stone Seen by Choledochoscope 3
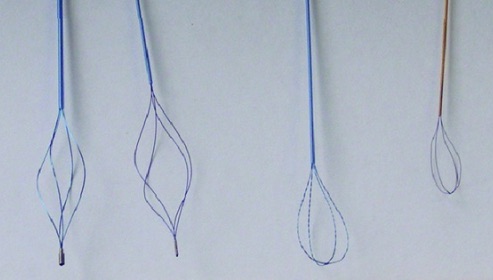
Various Wire Baskets 14
Open Common Bile Duct Exploration
Indications
- Choledocholithiasis During an Open Cholecystectomy
- Choledocholithiasis After Failure of Laparoscopic Common Bile Duct Exploration
- Choledocholithiasis if Endoscopy & Laparoscopy are Unavailable
Procedure
- Ligate Proximal Cystic Duct
- Choledochotomy Incision
- 5 cm Longitudinal Incision Just Above Duodenum
- Use Stay-Sutures on Either Side to Keep the Choledochotomy Open
- May Require Kocher Maneuver to Mobilize the Duodenum
- Retrieve Stones
- *See Below
- Consider T-Tube if Suspect Residual Stones or Concern for Stricture
- Close with Absorbable Monofilament Suture
Methods to Retrieve Stones
- Manual Expression
- Generally Preferred as the Initial Method
- Forceps Removal
- Classically Using Desjardins Gallstone Forceps
- Fogarty/Balloon Catheter
- Choledochoscope-Guided Wire Basket
Closure Options
- Primary Closure
- Use an Absorbable Monofilament Suture
- Historically Concerned for Risk of Biliary Stricture but Recently Being Disproven 11
- Closure Over a T-Tube
- Historically the Gold Standard Closure but Now Falling Out of Favor
- Increased Risk of Complications, Leaks, Longer Operating Time, and Longer Hospital Length of Stay 11,17
- Less Common Options:
- C-Tube (Through the Cystic Duct Stump)
- Antegrade Stenting
Postoperative Management of a T-Tube
- Repeat Cholangiogram at 24-48 Hours
- If Normal: Keep Clamped & Flush with Saline Once-Twice Per Day
- If Obstructed/Retained Stone: Leave Open to Drain
- Repeat Cholangiogram at 10-14 Days
- If Normal: Remove
- If Obstructed/Retained Stone: ERCP or IR Intervention per T-Tube
Options If Stone is Impacted and Unable to Remove
- Leave T-Tube
- Postoperative ERCP
- If Preoperative ERCP Failed:
- Transduodenal Sphincteroplasty
- Biliary-Enteric Drainage (Side-to-Side Choledochoduodenostomy)
Open Choledochotomy with Retention Sutures 15

Desjardins Gallstone Forceps
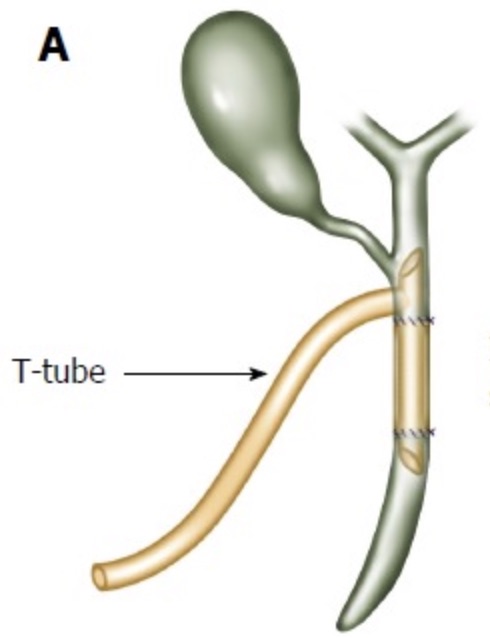
Biliary T-Tube 16
Transduodenal Sphincteroplasty
Definition
- Sphincteroplasty Performed in an Open Fashion Made through an Incision in the Duodenum
- *Fallen into Disuse with Modern Endoscopic Interventions
Indications
- Impacted Stone After Common Bile Duct Exploration (Generally Only if Postoperative ERCP is Otherwise Contraindicated – i.e. Failed Preoperatively)
- Sphincterotomy Otherwise Indicated but Endoscopic Approach is Contraindicated:
- Recurrent Stricture After Endoscopic Sphincterotomy
- Ampulla Endoscopically Inaccessible
- Pancreatic Divisum
Procedure
- Kocher Maneuver to Mobilize the Duodenum
- Longitudinal Duodenotomy On the Lateral Side
- Insert a Soft Catheter, Probe, or Right-Angle into the Common Bile Duct Through the Ampulla of Vater
- Use a Pott’s Scissors or Scalpel to Cut the Papilla at the 11 O’clock Position
- Cut 15 mm in Length
- Clear the Common Bile Duct Stone
- Suture the Bile Duct Wall to the Duodenal Mucosa
- Start with the Apical Suture and Continue Along the Sides in Interrupted Fashion
- Use a 4-0 or 5-0 Absorbable Monofilament Suture
- Close the Duodenotomy Transversely
![]()
Transduodenal Sphincteroplasty 18
References
- Singh AN, Kilambi R. Single-stage laparoscopic common bile duct exploration and cholecystectomy versus two-stage endoscopic stone extraction followed by laparoscopic cholecystectomy for patients with gallbladder stones with common bile duct stones: systematic review and meta-analysis of randomized trials with trial sequential analysis. Surg Endosc. 2018 Sep;32(9):3763-3776.
- Mohseni S, Bass GA, Forssten MP, Casas IM, Martin M, Davis KA, Haut ER, Sugrue M, Kurihara H, Sarani B, Cao Y, Coimbra R. Common bile duct stones management: A network meta-analysis. J Trauma Acute Care Surg. 2022 Nov 1;93(5):e155-e165.
- Li P, Zhang Z, Li J, Jin L, Han W, Zhang J. Diagnostic value of magnetic resonance cholangiopancreatography for secondary common bile duct stones compared with laparoscopic trans-cystic common bile duct exploration. Med Sci Monit. 2014 Jun 4;20:920-6. (License: CC BY-NC-ND 4.0)
- Haggerty S, Richardson W, Fanelli R, Brunt LM, Stefanidis D. Clinical Spotlight Review: Laparoscopic Common Bile Duct Exploration. SAGES. 2017.
- Lyass S, Phillips EH. Laparoscopic transcystic duct common bile duct exploration. Surg Endosc. 2006 Apr;20 Suppl 2:S441-5.
- Nathanson LK, O’Rourke NA, Martin IJ, Fielding GA, Cowen AE, Roberts RK, Kendall BJ, Kerlin P, Devereux BM. Postoperative ERCP versus laparoscopic choledochotomy for clearance of selected bile duct calculi: a randomized trial. Ann Surg. 2005 Aug;242(2):188-92.
- Bandyopadhyay SK, Khanna S, Sen B, Tantia O. Antegrade common bile duct (CBD) stenting after laparoscopic CBD exploration. J Minim Access Surg. 2007 Jan;3(1):19-25. (License: CC BY 2.0)
- Yokoyama K, Tanigawa N, Ogata A, Nagai T, Higashino M. Laparoscopic Technique and Initial Experiences of Choledocholithotomy Closure With Knotless Unidirectional Barbed Sutures After Surgery for Biliary Stone Disease. Surg Laparosc Endosc Percutan Tech. 2015 Aug;25(4):e129-33.
- Fernandez LC, Toriz A, Hernandez J, Sanchez N, Linares E, Zenteno M, Cuendis A, Olivares J, Guerrero G, Cervantes CF. Knotless choledochorraphy with barbed suture, safe and feasible. Surg Endosc. 2016 Aug;30(8):3630-5.
- Zhu J, Zhang Y, Gong J, Xiao W, Li Y. Closure of Choledochotomy With a Barbed Absorbable Suture After Laparoscopic Common Bile Duct Exploration. Am Surg. 2020 Dec 22:3134820982861.
- Podda M, Polignano FM, Luhmann A, Wilson MS, Kulli C, Tait IS. Systematic review with meta-analysis of studies comparing primary duct closure and T-tube drainage after laparoscopic common bile duct exploration for choledocholithiasis. Surg Endosc. 2016 Mar;30(3):845-61.
- Yin Z, Xu K, Sun J, Zhang J, Xiao Z, Wang J, Niu H, Zhao Q, Lin S, Li Y. Is the end of the T-tube drainage era in laparoscopic choledochotomy for common bile duct stones is coming? A systematic review and meta-analysis. Ann Surg. 2013 Jan;257(1):54-66.
- Jin M, Yoon YC, Wi JH, Lee YH, Han IY, Park KT. Intraoperative balloon angioplasty using fogarty artertial embolectomy balloon catheter for creation of arteriovenous fistula for hemodialysis: single center experience. Korean J Thorac Cardiovasc Surg. 2015 Apr;48(2):120-5. (License: CC BY-NC 3.0)
- Cordes J, Nguyen F, Lange B, Brinkmann R, Jocham D. Damage of stone baskets by endourologic lithotripters: a laboratory study of 5 lithotripters and 4 basket types. Adv Urol. 2013;2013:632790. (License: CC BY 3.0)
- Yang XW, Yang J, Li L, Yan XZ, Zhang BH, Shen F, Wu MC. The outcome of ipsilateral hemihepatectomy in mucin-producing bile duct tumors. PLoS One. 2014 Apr 11;9(4):e92010. (License: CC BY 4.0)
- Cheng Y, Xiong XZ, Zhou RX, Deng YL, Jin YW, Lu J, Li FY, Cheng NS. Repair of a common bile duct defect with a decellularized ureteral graft. World J Gastroenterol. 2016 Dec 28;22(48):10575-10583. (License: CC BY-NC 4.0)
- Gurusamy KS, Koti R, Davidson BR. T-tube drainage versus primary closure after open common bile duct exploration. Cochrane Database Syst Rev. 2013 Jun 21;(6):CD005640.
- Velez DR. Transduodenal Sphincteroplasty. The Operative Review of Surgery.