Trauma: Crash Laparotomy
Crash Laparotomy
Position & Prep
- Arms Extended
- Prepare from Chin to Knee
Operative Sequence
- 1. Access & Exposure
- 2. Temporary Bleeding Control
- 3. Exploration
- 4. Decision (Definitive Repair vs. Damage Control)
Access & Exposure
Access & Exposure
- Incision: Long Midline from Xiphoid to Pubis
- Major Pitfall: Iatrogenic Injury to Left Liver, Bowel or Bladder
- Options to Avoid Scars:
- Extend Incision Superiorly/Inferiorly to Enter Virgin Territory
- Chevron Incision (Bilateral Subcostal, Double Kocher, Rooftop)
- Mercedes Incision
- Enter Fast & Eviscerate Bowel Early
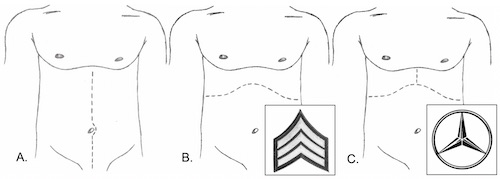
Incisions: (A) Midline, (B) Chevron, (C) Mercedes
Temporary Bleeding Control
Approach
- Blunt Trauma: Begin with Empirical Packing
- Penetrating Trauma: Begin by Directly Attacking the Bleeding
- *Some Recommend Empiric Packing in All Trauma Cases
Packing
- Pack Early – Relies on Ability to Form Clot
- Technique:
- “From Within” – Packed into a Cavity Applying Outward Pressure
- “From Without” – Create a Sandwich to Reapproximate Disrupted Tissue Planes
- Empiric Packing Sites:
- Right Side – Over/Under Liver & Along the Right Gutter
- Left Side – Over/Medial to Spleen & Along the Left Gutter
- Pelvis
Rapid Supraceliac Control (If Exsanguinating)
- Approach:
- Divide Gastrohepatic Ligament
- Normally Avascular
- Watch for Replaced Left Hepatic Artery
- Reflect Stomach/Esophagus to the Left to Visualize the Aorta
- May Require Division of the Diaphragmatic Crura
- Bluntly Dissect the Aorta
- Occlude Aorta Using:
- Manual Compress Against Spine
- Aortic Root Compressor/T-Bar
- Aortic Clamp – Consider Umbilical Tape to Hold Up
- Divide Gastrohepatic Ligament
- Clamp Distal Thoracic Aorta Through the Abdomen
- Thick Fibrous Attachments as Abdominal Aorta Passes Thorough Diaphragm
- Other Possible Options:
- Thoracotomy with Thoracic Aortic Control
- Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) – Controversial
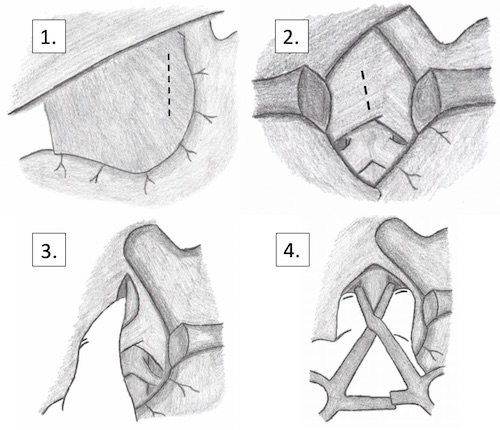
Supraceliac Control of the Aorta
Exploration
General Exploration
- Once Bleeding Temporarily Controlled
- Order of Exploration:
- 1. Inframesocolic
- 2. Supramesocolic
- 3. Lesser Sac
- 4. Retroperitoneum
- *Some Report Different Orders of Exploration – Exact Order is Not as Important as Making Sure to Preform it the Same Way Every Time & to Not Miss Any Injuries
Inframesocolic Exploration
- Lift Transverse Colon Cranially
- Run Bowel from Ligament of Treitz to Rectum
- Transverse Colon & Hepatic/Splenic Flexures are Notorious for Missed Injury
- Inspect Bladder & Pelvis
Supramesocolic Exploration
- Pull Transverse Colon Caudally
- Inspect from Right-to-Left
- Palpate Liver, Gallbladder & Right Kidney
- Then Stomach & Duodenum
- Finally, Palpate Spleen & Left Kidney
Lesser Sac Exploration
- Bluntly Dissect Through the Greater Omentum (Left Side Less Vascular)
- Inspect Posterior Stomach & Pancreas
Retroperitoneum Exploration
- Keep Retroperitoneal Exploration Targeted & Limited
- Clinical Suspicion Based on Missile Trajectory or Presence of Hematoma
- Maneuvers:
- Mattox
- Cephalad Transverse Mesocolon Reflection
- Kocher
- Cattell-Braasch
- *Understand that There is Significant Overlap with the Maneuvers & They Should be Tailored to the Individual Patient
- *See General Abdomen: Maneuvers & Retroperitoneal Exposure
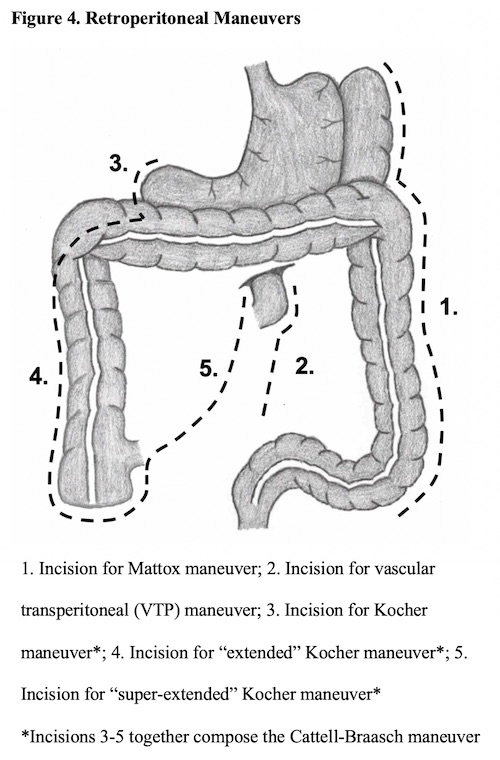
Maneuvers to Access the Retroperitoneum
Decision (Definitive Repair vs. Damage Control)
Damage Control Definition
- Definition: Surgery to Stabilize with Delayed Definitive Repair
- Goals:
- Arrest Hemorrhage
- Limit Contamination
- Maintain Blood Flow
- Temporary Abdominal Closure
- Operative Time Limited to Minimize Further Hypothermia, Coagulopathy and Acidemia
Damage Control Indications
- Severe Physiologic Insult
- Acidosis (pH < 7.2)
- Base Deficit > 14-15
- Lactate > 5
- Temp < 34-35
- Coagulopathy (Clinical Evidence or INR > 1.5)
- Intraoperative Ventricular Arrhythmia
- High Blood Loss
- Unable to Control Bleeding by Conventional Methods
- Blood Loss > 4 L
- Blood Transfusion > 10 U
- Injury Pattern
- 5 Different Injury Patterns
- Difficult to Assess Major Venous Injury
- Massive Hemorrhage from the Pancreatic Head
- Major Liver or Pancreaticoduodenal Injury with Hemodynamic Instability
- Pancreaticoduodenal Devascularization or Massive Disruption with Involvement of Ampulla or Distal CBD
- Need for Staged Reconstruction
- Need to Reassess Bowel Viability
- Unable to Close Abdominal Wall Without Tension
- Signs of Abdominal Compartment Syndrome While Attempting Closure
Damage Control Phases
- DC-0: Preoperative
- DC-I: Initial Operation
- DC-II: Resuscitation
- DC-III: Definitive Repair
- DC-IV: Delayed Soft Tissue Reconstruction (If Needed)