Consider Incision of Peripheral Attachments and Reattachment 2-3 Interspaces More Cephalad
For Complete Avulsion: Reattach to Ribs
Place Sutures Circumferentially Around the Ribs
May Also Consider Using Rib Suture Anchors
Timing/Approach:
Immediate Dx (< 1 Week): Transabdominal Approach
Delayed Dx (> 1 Week): Transthoracic Approach
To Evaluate Viscera & Adhesions
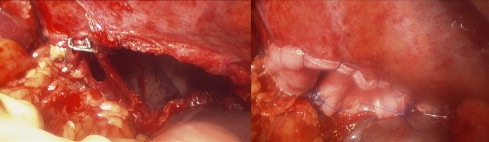
Diaphragm Laceration & Repair 1
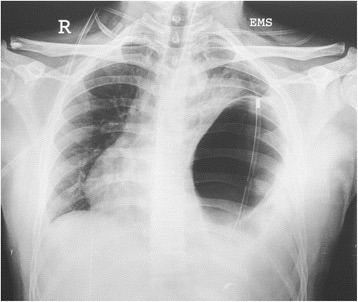
Traumatic Diaphragmatic Hernia on CXR 2
References
Pakula A, Jones A, Syed J, Skinner R. A rare case of chronic traumatic diaphragmatic hernia requiring complex abdominal wall reconstruction. Int J Surg Case Rep. 2015;7C:157-60.(License: CC BY-NC-ND-3.0)
Vyas PK, Godbole C, Bindroo SK, Mathur RS, Akula B, Doctor N. Case-based discussion: an unusual manifestation of diaphragmatic hernia mimicking pneumothorax in an adult male. Int J Emerg Med. 2016 Dec;9(1):11. (License: CC BY-4.0)
The most effective and up-to-date oral board review book available. Focused on diagnosis and treatment in bullet-point format, this book will help you formulate a reasonable and safe approach to surgical pathology and master your oral boards.
100% of profits are directed back into the program to fund further initiatives at improving surgical resident training.