Difficult Abdominal Closure
Difficult Abdominal Closure
David Ray Velez, MD
Table of Contents
Concept
Damage Control Laparotomy (DCL), Required for Abdominal Injury or Peritonitis Due to Abdominal Sepsis, May Result in Loss of Domain with an Inability to Achieve Primary Myofascial Closure
Both Abdominal Pathology and the Resulting Massive Resuscitation Cause Significant Edema of the Bowel, Retroperitoneum, and Abdominal Wall with Lateral Muscle Contraction and Loss of Compliance
Approach and Adjuncts
Damage Control Laparotomy (DCL) with an Open Abdomen (OA) is Initially Managed with Temporary Abdominal Closure (TAC) Until Hemodynamically Stable and the Intraabdominal Pathology Has Resolved
Once Appropriate for Closure, Primary Abdominal Closure is Preferred as Soon as Possible if Able
Attempts to Achieve Primary Closure if Initially Unable
- Prolonged Monitoring – Repeated Returns to the Operating Room for Exchange of Temporary Abdominal Closure (TAC) Device Until Edema Resolves and the Fascia Can Close
- Fascial Traction Techniques – *See Techniques Below
- Component Separation – Generally Not Done in the Acute Care Setting, Planes are Rather Spared and Saved for a Delayed Repair Later Once the Patient Fully Recovers
Options if Unable to Close Fascia Primarily
- These Options Accept the Resulting Large Ventral Hernia with Plan for Abdominal Wall Reconstruction Later Under More Favorable Terms Once the Patient is Fully Recovered
- Skin-Only Closure – Closure of Only the Skin
- Delayed Skin Grafting – Can Either Place an Underlying Bridging Mesh or Use a WVAC to Form Granulation Tissue Prior to Grafting
- Least Favorable Option but Done if Unable to Even Close the Skin
- Bridging Mesh – Use of an Absorbable Mesh to Temporarily Bridge the Fascial Defect
- Prefer Overlying Skin-Only Closure if Able or Else Plan for Delayed Skin Grafting
A 2022 EAST Guideline Conditionally Recommends the Use of Fascial Traction Systems in Hemodynamically Normal Trauma and Emergency General Surgery Patients Once the Intra-Abdominal Pathology Has Been Addressed – Increased Rate of Primary Fascial Closure with No Change in Mortality or Enterocutaneous Fistula (ECF) Rates
Adjuncts to Reduce Visceral Edema
- Negative Pressure Wound Therapy (NPWT/Abthera) – Continuously Drains Exudate and Decreases Edema
- Furosemide (Lasix) – Appropriate Diuresis Can Be Attempted Once Hemodynamically Stable and the Intraabdominal Pathology Has Resolved
- Although Routinely Used There is No Significant Data to Support Increased Rates of Fascial Closure or Improved Outcomes
- Direct Peritoneal Resuscitation (DPR) – Instillation of Dialysate into the Peritoneal Cavity to Improve Blood Flow and Decrease Inflammation and Edema
- A Newer Technique that Seems Promising but There is Insufficient Data to Make Any Definitive Recommendations

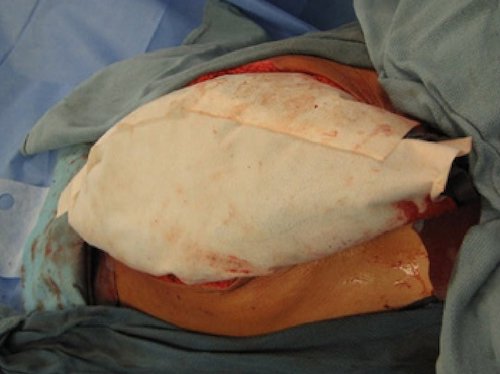
Temporary Abdominal Closure (TAC) 1

Delayed Skin Grafting 2
Fascial Traction Techniques
The Goal of Fascial Traction Techniques are to Provide Continuous Traction to Stretch the Abdominal Wall Over Time and Eventually Allow Primary Fascial Closure
Fascial Traction Systems are Generally Performed Along with Negative Pressure Wound Therapy (NPWT/Abthera) to Protect Underlying Bowel and Drain Exudate
Timing
- Facial Traction Systems Can Be Employed Once a Patient is Hemodynamically Stable and the Intraabdominal Pathology Has Resolved
- Allow for Repeated Fascial Tightening at Set Intervals Every 24-48 Hours Until Fascia Can Be Closed Primarily without Significant Tension
- Generally Require 2-4 Tightenings
There are Multiple Systems Available to Provide Fascial Traction but None Have Definitively Proven to Be Superior
Wittmann Patch – Two Velcro (Hook and Loop) Sheets are Sutured to the Fascial Edges and Progressively Tightened Over a Period of Time Until the Sheets Can Be Removed and Fascia Closed Primarily
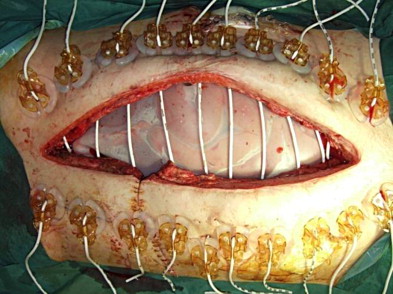
Transabdominal Wall Traction (TAWT) – Uses a Whittmann Patch Attached to the Underside of the Abdominal Wall, Lateral to the Rectus Muscle with Sutures Brought Through the Skin to a Bolster
- Will Develop Pressure Injuries at the Bolster Sites
Mesh-Mediated Fascial Traction (MMFT) – Two Sheets of Permanent Polypropylene Mesh are Sutured to the Fascial Edges and Progressively Tightened Over a Period of Time Until the Sheets Can Be Removed and Fascia Closed Primarily
- Alternatively: Can Place a Single Mesh Circumferentially and “Pinch” at Set Intervals to Evaluate for Laxity – If Laxity Has Developed the Excess Mesh is Sutured to Maintain Traction
Bogota Bag-Mediated Fascial Traction – Two Sterile IV Fluid Bags are Sutured to the Fascial Edges and Progressively Tightened Over a Period of Time Until the Sheets Can Be Removed and Fascia Closed Primarily
Canica ABRA System – Multiple Elastic Bands are Passed Through Each Side of the Abdominal Wall and Progressively Tightened Over a Period of Time Until the Bands Can Be Removed and Fascia Closed Primarily
Progressive Partial Fascial Closure – Fascial Sutures Are Placed in an Interrupted Fashion Until Tension Develops and Return to the Operating Room at Set Intervals to Place Additional Sutures as Able Until Closed
Whitmann Patch 2

Transabdominal Wall Traction (TAWT)
Canica ABRA System 3
References
- Alvarez PS, Betancourt AS, Fernández LG. Negative Pressure Wound Therapy with Instillation in the Septic Open Abdomen Utilizing a Modified Negative Pressure Therapy System. Ann Med Surg (Lond). 2018 Oct 10;36:246-251. (License: CC BY-4.0)
- Huang Q, Li J, Lau WY. Techniques for Abdominal Wall Closure after Damage Control Laparotomy: From Temporary Abdominal Closure to Early/Delayed Fascial Closure-A Review. Gastroenterol Res Pract. 2016;2016:2073260. (License: CC BY-4.0)
- Iype S, Butler A, Jamieson N, Middleton S, Jah A. Delayed dynamic abdominal wall closure following multi-visceral transplantation. Int J Surg Case Rep. 2014;5(12):988-91. doi: 10.1016/j.ijscr.2014.08.006. (License: CC BY-NC-ND-3.0)