Diverticulitis 1
Modified Hinchey Class 0 2

Diverticulitis Hinchey Class I 3
Diverticulitis Hinchey Class II 2
Diverticulitis Hinchey Class III/IV 4
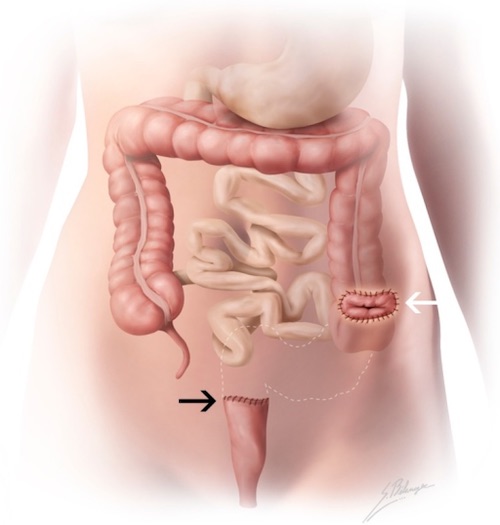
Hartmann Procedure 5
Diverticulitis 1
Modified Hinchey Class 0 2
Diverticulitis Hinchey Class I 3
Diverticulitis Hinchey Class II 2
Diverticulitis Hinchey Class III/IV 4
Hartmann Procedure 5