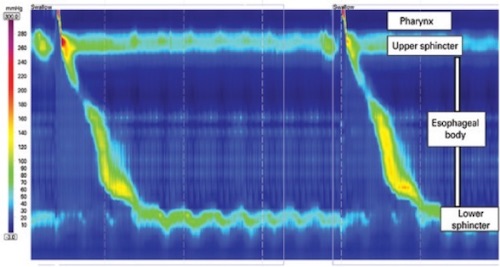
Normal Manometry 1
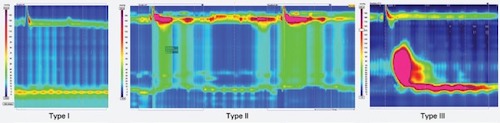
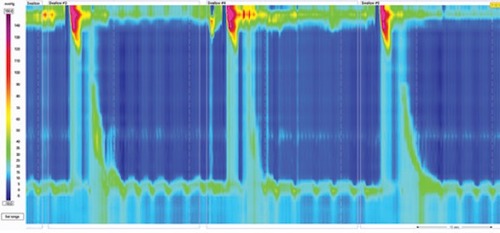
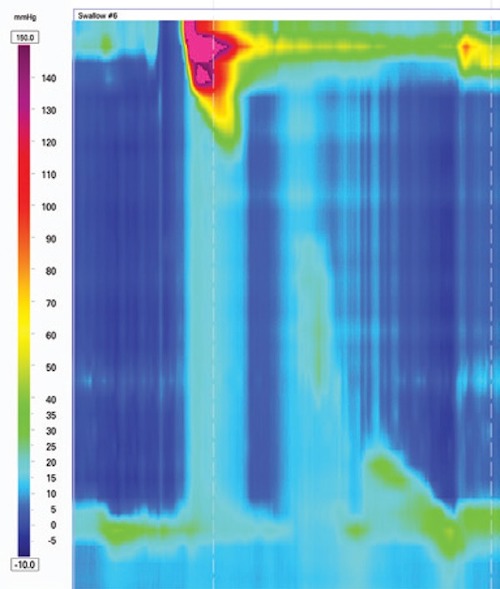
Achalasia Manometry; Type I – No Contractility with Incomplete LES Relaxation; Type II – Penesophageal Pressurization; Type III – Premature Spastic Contractions 1
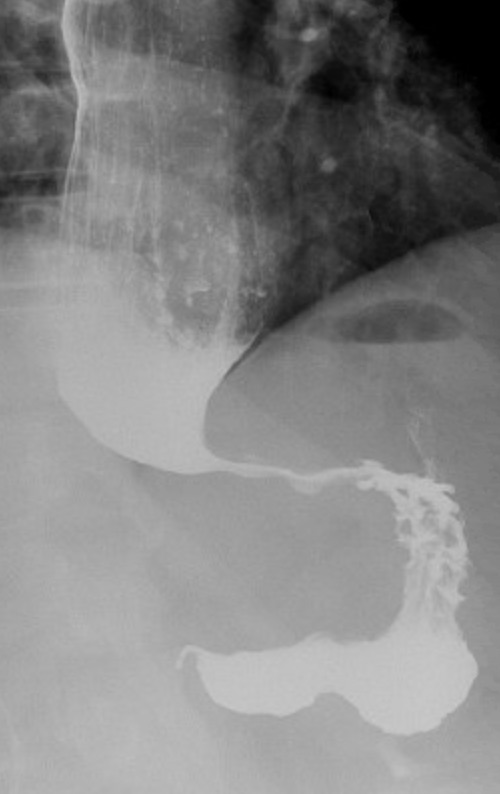
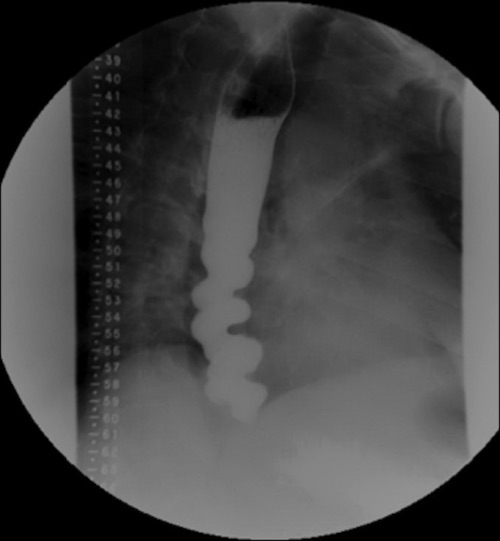
“Birds Beak” on Esophagram
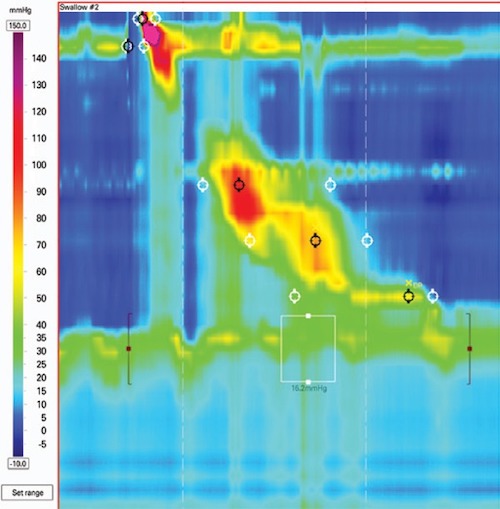
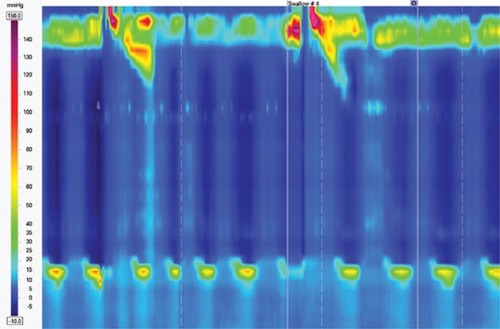
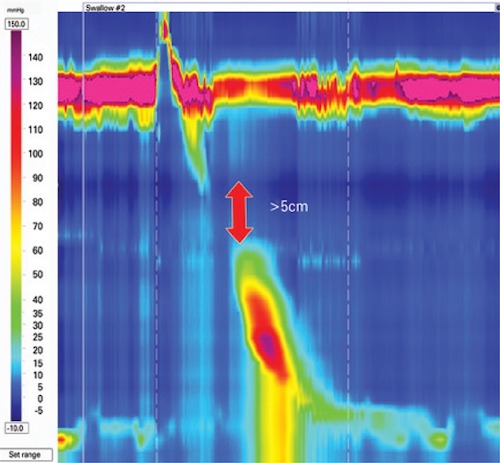
EGJOO Manometry 1
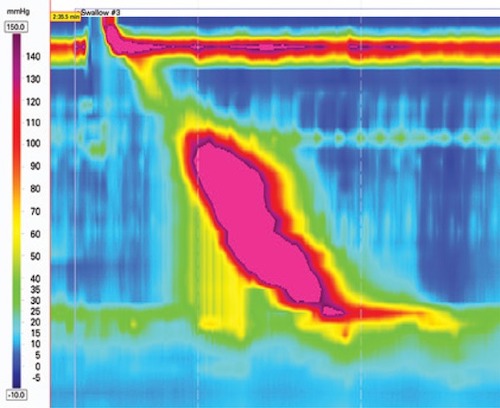
DES Manometry 1
“Corkscrew” on Esophagram 2
Hypercontractile Esophagus Manometry 1
Absent Contractility Manometry 1
IEM Manometry 1
Fragmented Peristalsis Manometry 1