Small Bites (5-7 mm Every 5-7 mm) – Largely Based on the STITCH Trial
Goal Suture:Wound Length: 4:1
Suture Selection
Slowly Absorbable Monofilament Suture is Generally Preferred
2-0 PDS Was Used in the Classic STITCH Trial
Barbed Suture (Stratafix, V-Loc) May Decrease the Risk of Fascial Dehiscence and Evisceration
Triclosan-Coated Suture (Stratafix Symmetric, PDS Plus) May Decrease the Rates of Surgical Site Infections
Prophylactic Mesh Placement
May Decrease the Risk of Hernia
Onlay or Retro-Muscular Plane is Preferred
Complications:
Increased Risk of Seroma
No Increased Risk of Infection
*Use is Debated and Not Clearly Defined
Abdominal Binders
No Evidence to Show Decreased Risk of Incisional Hernia or Burst Abdomen
May Decrease Postoperative Pain
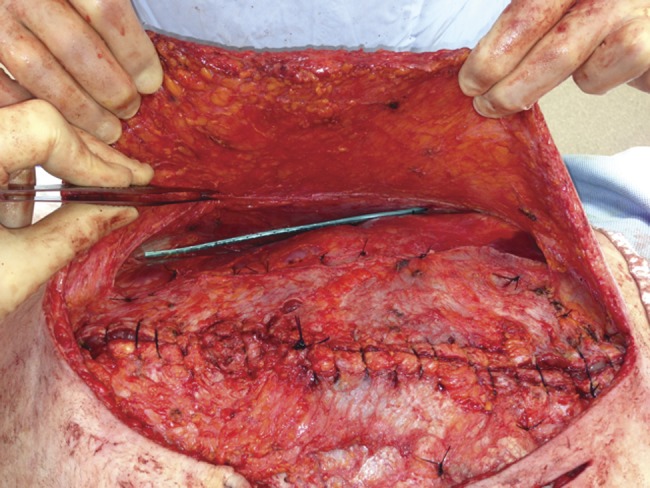
Fascial Closure 1
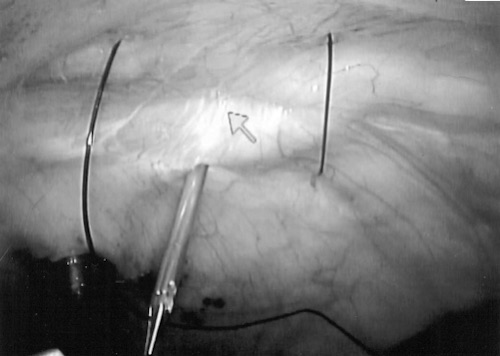
Port-Site Closure
Indications to Close the Fascial Defect
Trocar Sites ≥ 10 mm
Any Size After Single-Incision Laparoscopic Surgery (SILS)
Any Size at the Umbilical Site
Technique for Port-Site Closure
Over 20+ Techniques Have Been Described but There are Three General Groups
Intracorporeal Assistance – Require 2 Additional Ports (One to Visualize and One to Manipulate)
Maciol Needles
Grice Needles
Endoclose Suture Device
Extracorporeal Assistance – Require One Additional Port to Visualize
Carter-Thomason CloseSure System
Endo-Judge Wound Closure Device
Tahoe Surgical Instrument Ligature Device
External Closure – No Additional Ports Required
Suture Carrier
Dual-Hemostat Technique
Standard Hand Suture Closure
Carter-Thomason Device 2
References
Rawstorne E, Smart CJ, Fallis SA, Suggett N. Component separation in abdominal trauma. J Surg Case Rep. 2014 Jan 20;2014(1):rjt133. (License: CC BY-NC-3.0)
Eid GM, Thodiyil PA, Collins J, Bonanomi G, Mattar SG, Hughes SJ, Schauer PR, Wilson M. Laparoscopic repair of umbilical hernias in conjunction with other laparoscopic procedures. JSLS. 2006 Jan-Mar;10(1):63-5. (License: CC BY-NC-ND-3.0)