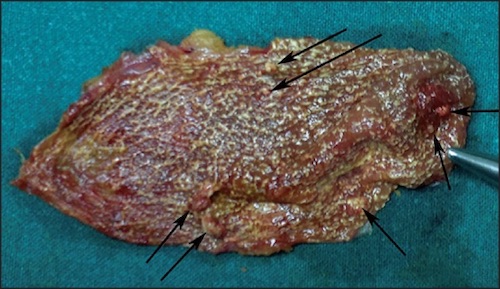
Cholesterolosis of the Gallbladder 1
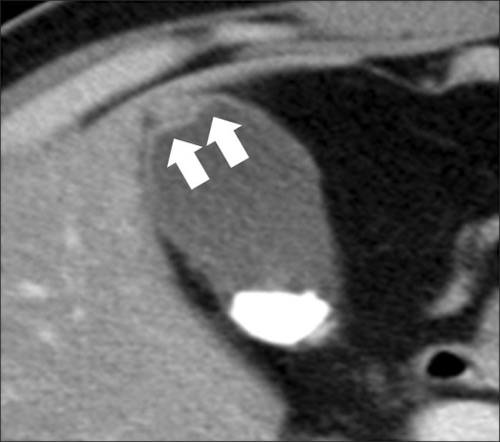
Adenomyomatosis of the Gallbladder 2
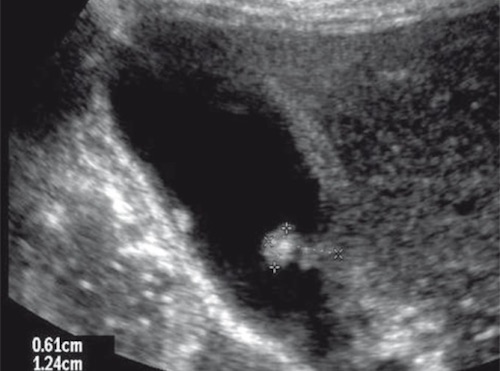
Gallbladder Polyp on US 3
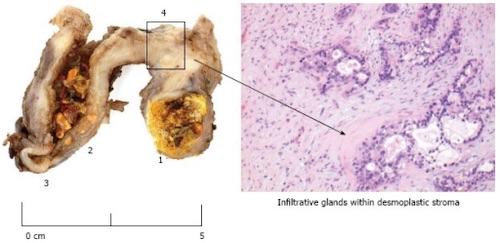
Gallbladder Carcinoma 4
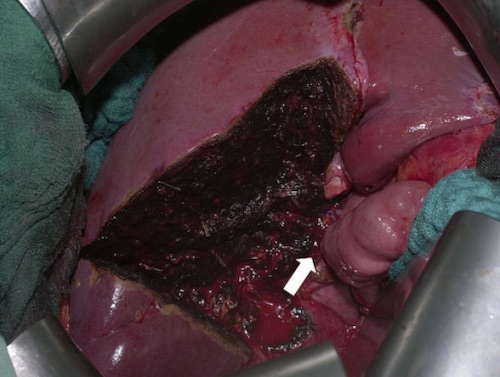
Formal Segment IVb & V Liver Resection 5
Cholesterolosis of the Gallbladder 1
Adenomyomatosis of the Gallbladder 2
Gallbladder Polyp on US 3
Gallbladder Carcinoma 4
Formal Segment IVb & V Liver Resection 5