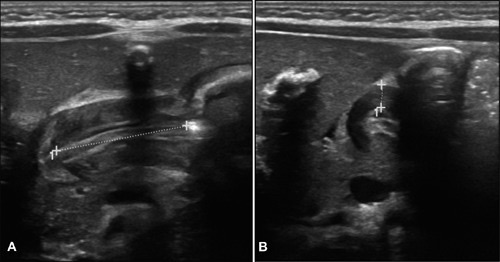
Pyloric Stenosis on US; 20 mm Length (a), 5 mm Thick (b) 1
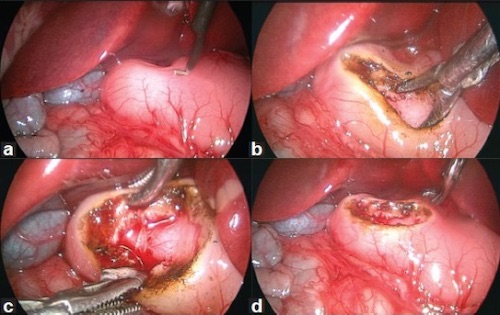
Pyloromyotomy; (a) Muscle Hypertrophy, (b-c) Muscle Separation, (d) Completed Myotomy 2
Pyloric Stenosis on US; 20 mm Length (a), 5 mm Thick (b) 1
Pyloromyotomy; (a) Muscle Hypertrophy, (b-c) Muscle Separation, (d) Completed Myotomy 2