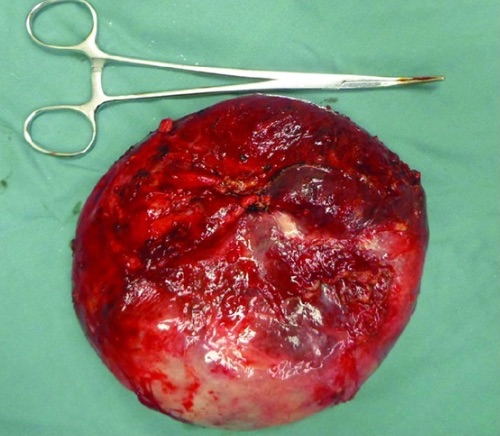
Multilocular, > 10 cm or High Rupture Risk: Surgical Excision (Need Entire Wall)
*May Consider PAIR (Puncture, Aspiration, Injection, Reaspiration) if Unilocular 5-10 cm
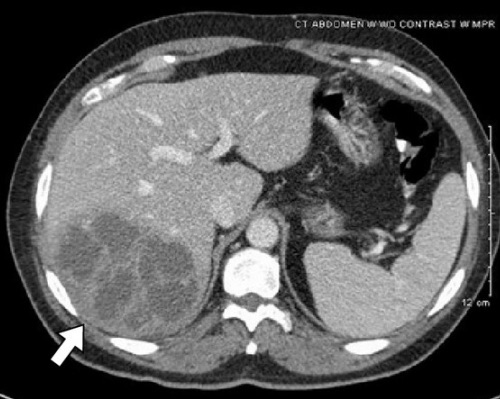
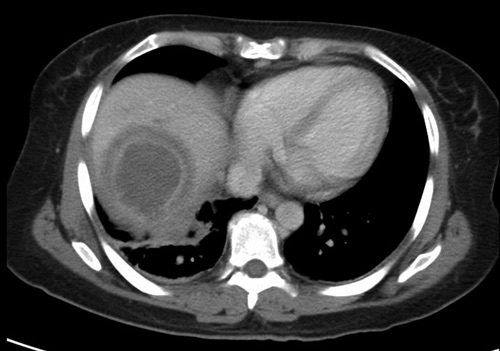
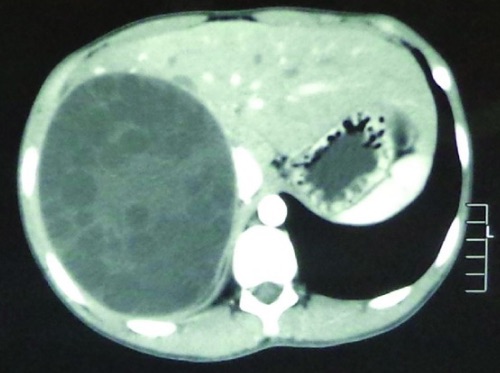
Hydatid Cyst of the Liver 3
Hydatid Cyst of the Liver 3
Fungal Abscess
Basics
Most Common in Immunocompromised (Often Following Chemotherapy for Hematologic Malignancy)
Most Common Fungi:
Candida – Most Common
Aspergillus
Cryptococcus
Often Mixed Fungi & Bacteria
Presentation:
Fever
Jaundice
RUQ Pain
Treatment
Primary Tx: Percutaneous Drainage & Antifungals
First-Line Antifungals: Micafungin or Caspofungin
Mnemonics
Entamoeba vs Echinococcus Abscesses
“Mexican Fire Ants & Bent Rhino Horns”
Amebic/Entamoeba:
Mexican: “Mexico Connection”
Fire: (F-F) Flagyl Treatment
Ants: (A-A) Amebic & (Ant:Ent) Entamoeba
Hydatid/Echinococcus:
Bent: Al-BEND-azole
R-HINO: Ec-HINO-coccus
Horns: (H-H) Hydatid
References
Livingston LV, Perez-Colon E. Streptococcus intermedius Bacteremia and Liver Abscess following a Routine Dental Cleaning. Case Rep Infect Dis. 2014;2014:954046. (License: CC BY-3.0)
Garvin KW, Willig JH. Amebic liver abscess. Am J Trop Med Hyg. 2010 Nov;83(5):961. (License: CC BY-2.5)
Ma Z, Yang W, Yao Y, Liu Q. The adventitia resection in treatment of liver hydatid cyst: a case report of a 15-year-old boy. Case Rep Surg. 2014;2014:123149. (License: CC BY-3.0)