
Melanoma 1

Lentigo Maligna 2
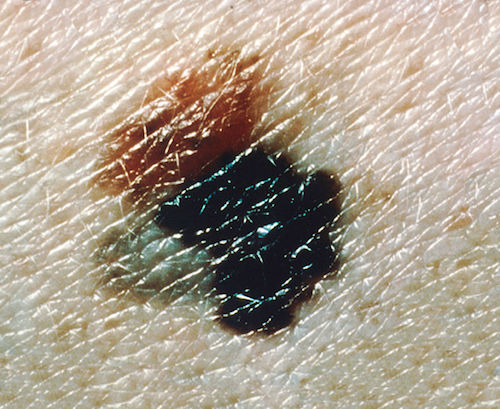
Superficial Spreading 1

Acral Lentiginous 3

Subungual 4

Nodular 5
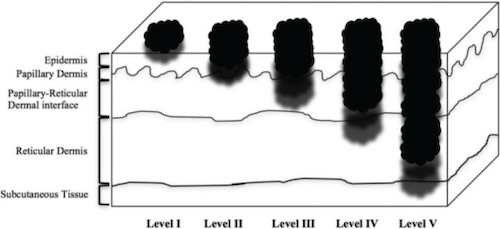
Melanoma Clark Level 6
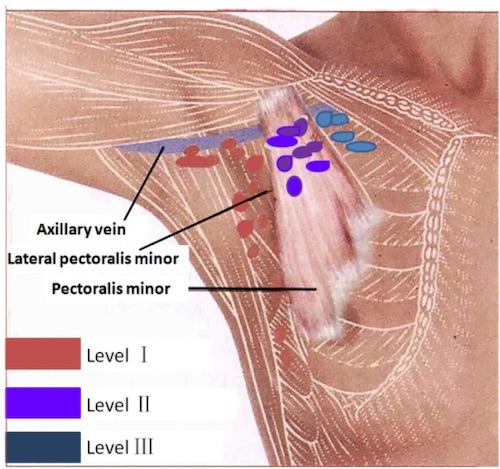
Axillary Lymph Node Levels 7
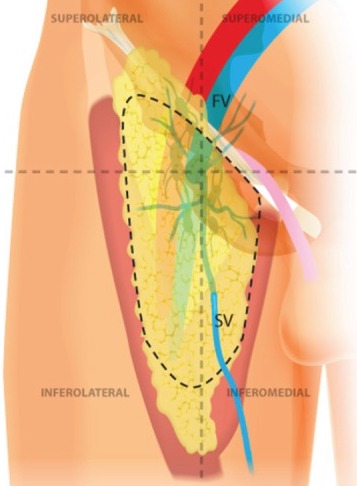
Superficial Groin Dissection 8
Melanoma 1
Lentigo Maligna 2
Superficial Spreading 1
Acral Lentiginous 3
Subungual 4
Nodular 5
Melanoma Clark Level 6
Axillary Lymph Node Levels 7
Superficial Groin Dissection 8