Definition: A Rare Fluid-Filled Cavity within the Mesentery
Believed to be Caused by Ectopic Lymphatic Proliferation that Fails to Communicate with Lymphatic System Due to Trauma, Infection, or Neoplasia (Exact Etiology is Not Certain)
Presentation
Nonspecific Symptoms, Often Found Incidentally
Abdominal Pain
Nausea and Vomiting
Constipation
Diarrhea
May Have a Palpable Abdominal Mass
Fluid Content is Generally Straw-Colored and Proteinaceous with High Triglycerides but May be Hemorrhagic, Serous, Chylous, or Infected
Location
Small Bowel (60%)
Large Bowel (24%)
Retroperitoneum (14.5%)
May Be Seen on CT but Diagnosis is Confirmed by Histopathology After Excision
Treatment
The Primary Treatment is Surgical Excision – Prevent Recurrence or Malignant Transformation
If Vasculature is Not Compromised: Simple Enucleation and Closure of the Mesenteric Defect
If Vasculature is Compromised: Resection of the Mesentery and Associated Bowel
Mesenteric Cyst at Laparoscopy 1
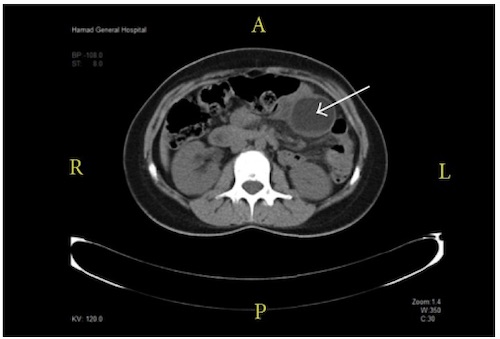
Mesenteric Cyst (Arrow) on CT 1
Mesenteric Tumor
Types
Lymphoma – The Most Common Mesenteric Malignancy
Classic “Sandwich” Appearance on CT (Lymphadenopathy Surrounding Mesenteric Vessels)
Cystic Lymphangioma – The Most Common Mesenteric Cystic Tumor
Lipoma
Liposarcoma
Desmoid Tumor
Fibroma
Inflammatory Pseudotumor
Actinomycosis
Mesothelioma
Pseudocyst
Tumors at the Root of the Mesentery are More Likely to Be Malignant
Presentation
Nonspecific Symptoms, Often Found Incidentally
Abdominal Pain
Nausea and Vomiting
Constipation
Diarrhea
May Have a Palpable Abdominal Mass
Diagnosis
Imaging (CT/MRI) May Be Diagnostic for Certain Cystic Tumors or Desmoid Tumors
Definitive Diagnosis Most Often Requires Histopathologic Examination (Either Biopsy or Surgical Resection)
Biopsy Can Be Achieved by Fine Needle Aspiration (FNA) or Core Needle Biopsy (CNB)
FNA is Preferred for Small Masses, Cystic Masses, or Masses Close to Vasculature
CNB is Preferred for Large Solid Masses
Either Ultrasound or CT-Guided
Management
Management Varies by Tumor Type
The Primary Treatment is Surgical Resection for the Majority of Tumors
Well-Circumscribed Tumors May Be Amenable for Simple Enucleation
More Invasive Tumors May Require Wider Resection and Associated Bowel Resection if Vasculature is Compromised – Caution to Avoid Short Bowel Syndrome
Lymphoma is Primarily Managed by Chemotherapy
Symptomatic or Malignant Appearing Tumors are Often Resected without Preoperative Biopsy
Malignant Appearing Tumors that are Unresectable Should Have a Biopsy to Confirm Diagnosis Prior to Chemotherapy/Radiation
Benign Appearing Tumors that are Asymptomatic Have Variable Management – Surveillance vs. Biopsy vs. Resection
Peritoneal Carcinomatosis: Cytoreductive Surgery (CRS) and HIPEC if Appropriate
Abdelaal A, Sulieman I, Aftab Z, Ahmed A, Al-Mudares S, Al Tarakji M, Almuzrakchi A, Toro A, Di Carlo I. Laparoscopy as a Diagnostic and Definitive Therapeutic Tool in Cases of Inflamed Simple Lymphatic Cysts of the Mesentery. Case Rep Surg. 2015;2015:325939. (License: CC BY-3.0)
Rami M, Mahmoudi A, El Madi A, Khalid, Khattala, Afifi MA, Bouabdallah Y. Giant cystic lymphangioma of the mesentery: varied clinical presentation of 3 cases. Pan Afr Med J. 2012;12:7. (License: CC BY-2.0)