Can Be Evaluated in the OR if Unstable or There for Other Reasons
Small: Repair Transversely in 1-Layer with Absorbable Suture
2-Layers Risk Stenosis
Include Tracheal Rings in Repair
Large: Primary Anastomosis (Up to 5-6 Tracheal Rings in Length)
Strongly Consider Tracheostomy – Place in Standard Position or Possibly Through the Injured Site
Recurrent Laryngeal Nerve
Tx: Repair or Re-Implant in Cricoarytenoid Muscle
Thyroid
Tx: Control Bleed & Drain (No Resection)
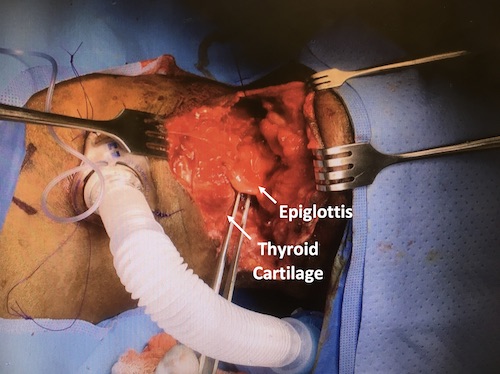
Larynx Laceration
References
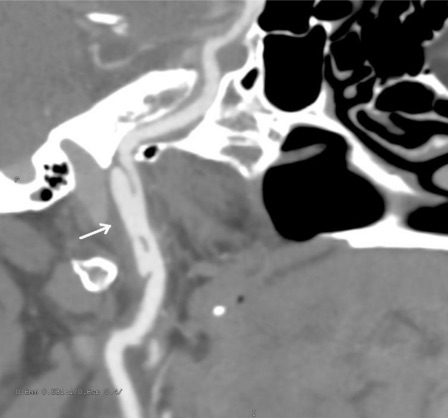
Karamchandani R, Rajajee V, Pandey A. The role of neuroimaging in the latent period of blunt traumatic cerebrovascular injury. Open Neuroimag J. 2011;5:225-31. (License: CC BY-NC-3.0)
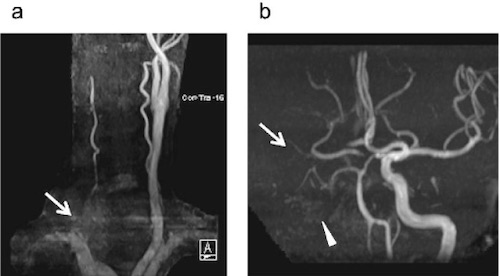
Kobayashi K, Imagama S, Okura T, Yoshihara H, Ito Z, Ando K, Ukai J, Shinjo R, Muramoto A, Matsumoto T, Nakashima H, Ishiguro N. Fatal case of cervical blunt vascular injury with cervical vertebral fracture: a case report. Nagoya J Med Sci. 2015 Aug;77(3):507-14.(License: CC BY-NC-ND-4.0)
Babu A, Garg H, Sagar S, Gupta A, Kumar S. Penetrating neck injury: Collaterals for another life after ligation of common carotid artery and subclavian artery. Chin J Traumatol. 2017 Feb;20(1):56-58. (License: CC BY-NC-ND-4.0)