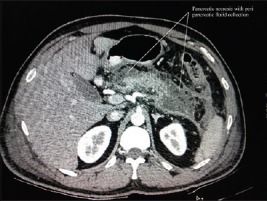
Heterogenous Fluid Density – Some Solid Components
No Defined Wall
Intrapancreatic or Extrapancreatic
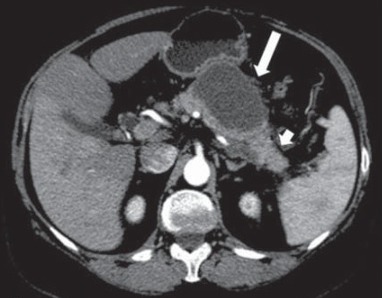
Walled-Off Pancreatic Necrosis (WOPN)
> 4 Weeks
Heterogenous Fluid Density
Well Defined Wall
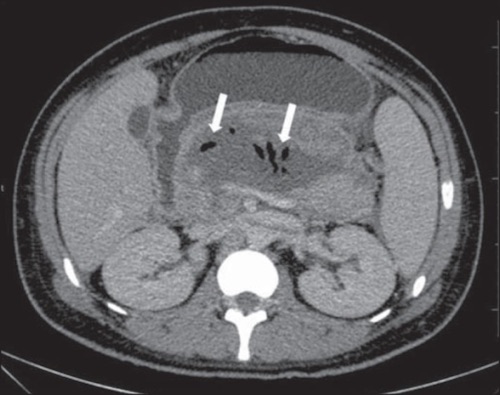
Diagnosis of Infection
CT Showing Gas within the Necrosis (Highly Specific but Not Sensitive)
Percutaneous Needle Aspiration Should Be Considered for Prolonged Illness if CT is Not Specific – May Consider Forgoing if Planning to Treat Empirically & Aspiration Will Not Change Management
Acute Necrotic Collection 2
Walled-Off Pancreatic Necrosis 3
Infected Pancreatic Necrosis 4
Treatment
Sterile Pancreatic Necrosis
Primary Treatment: Medical Therapy (No Antibiotics Necessary)
Surgical Debridement:
Indications:
Failure to Thrive
Persistent Abdominal Pain
Worsening Organ Failure
Should Be Delayed Until 30 Days After Diagnosis
Mortality:
< 15 Days: 75%
15-29 Days: 45%
≥ 30 Days: 8%
Infected Pancreatic Necrosis
Stable: “Step-Up Approach”
Unstable: Antibiotics & Open Necrosectomy
Use Blunt Finger Dissection – Best to Differentiate Live vs Necrotic Tissue
“Step-Up Approach”
Approach for Management of Infected Necrotizing Pancreatitis
Pandiaraja J. Another cutaneous sign of acute pancreatitis. Indian J Crit Care Med. 2016 May;20(5):313-4. (License: CC BY-NC-SA-3.0)
Cunha EF, Rocha Mde S, Pereira FP, Blasbalg R, Baroni RH. Walled-off pancreatic necrosis and other current concepts in the radiological assessment of acute pancreatitis. Radiol Bras. 2014 May-Jun;47(3):165-75. (License: CC BY-NC-3.0)
Cunha EF, Rocha Mde S, Pereira FP, Blasbalg R, Baroni RH. Walled-off pancreatic necrosis and other current concepts in the radiological assessment of acute pancreatitis. Radiol Bras. 2014 May-Jun;47(3):165-75. (License: CC BY-NC-3.0)