Parastomal Hernia
Parastomal Hernia
Duncan G. Hartley, MD
Table of Contents
Definition
Parastomal Hernia: Protrusion of Intestine Through the Fascial Opening into the Subcutaneous Tissue Around a Stoma
Incidence: 30-50%
Most Develop within the First 2 Years of Creation
- Only 20% Progress to Requiring Repair

Parastomal Hernia 1
Risk Factors
Most Common After: End Colostomy
Least Common After: Loop Ileostomy
- May Be Due to Their Frequently Temporary Nature
Patient Factors
- Obesity
- Poor Muscle Tone
- Chronic Cough
- Chronic Constipation
- Malnutrition
- Advanced Age
- Corticosteroid Use
- Ascites
Surgical Factors
- Placement Outside of Rectus Muscle
- Oversized Fascial Opening
- Excessive Splitting/Stretching of Muscle
- Emergency Surgery
Mesh at Index Operation Decreases Risk
Complications
Can Interfere with Pouch Appliance Adherence and Cause Leakage with Peristomal Wound Issues
Risk for Bowel Obstruction Causing Abdominal Pain, Distention, Nausea, and Vomiting
Risk for Bowel Incarceration and Strangulation – Similar to Other Abdominal Wall Hernias
Management
Consider Elective Reversal/Takedown if Feasible
The Majority are Managed Conservatively
- Ostomy/Stoma Belt (Support Binder) Worn When Expecting Episodes of Prolonged Increased Intraabdominal Pressure (Physical Activity, Lifting, etc.)
- Goal: Keep Appliance in a Stable Position to Prevent Leakage/Skin Damage (Not to Reduce the Hernia Itself)
- Weight Loss
- Diet Modification and Laxative/Stool Softener Use to Prevent Constipation
Emergent Surgical Repair Indications:
- Incarceration/Strangulation
- Bowel Obstruction that Has Failed Nonoperative Management
Elective Surgical Repair Considered for Chronic Moderate-Severe Symptoms that Fail to Improve with Conservative Management
Surgical Approach
- Prosthetic Mesh Repair
- Often the Preferred Approach with Decreased Recurrence Rates (But Still High 10-30%)
- Consider Biologic Mesh or Other Approaches if Prosthetic Mesh is Contraindicated (Active Infection or Gross Contamination)
- Primary Repair
- Generally Avoided Due to High Recurrence Rates (~ 70%)
- Stoma Relocation
- Generally Avoided Due to Persistently High Recurrence Rates
- May Be Required for Recurrent Hernias that Have Failed Prior Mesh Repair
- All Approaches Have High Risk of Recurrence up to 30% or Higher
Mesh Repair Techniques
Onlay Mesh Repair
- Midline Incision Made Down to the Fascia and then Carried Laterally with Subcutaneous Dissection Around the Stoma (Sparing the Current Mucocutaneous Junction)
- Hernia is Then Reduced, and a Tension-Free Mesh is Used to Close the Defect
Intraperitoneal Mesh Repair
- Can Be Done Open or Minimally Invasive (Laparoscopic/Robotic)
- After Abdominal Access, the Hernia is Reduced and Mesh is Applied (Sugarbaker or Keyhole Techniques)
- Sugarbaker Technique
- Bowel is Secured to the Anterior/Lateral Abdominal Wall
- Intraperitoneal Mesh is then Placed Over the Bowel Loop, Circumferentially Covering the Entire Fascial Defect
- Keyhole Technique
- A 2-3 cm Keyhole is Cut-Out from the Center of the Mesh
- Intraperitoneal Mesh is then Secured Around the Bowel to Cover the Entire Fascial Defect
Sublay (Retrorectus) Mesh Repair
- *Newest Technique
- Generally Performed Open Although Robotic Sublay Repair is Possible
- Dissect the Retrorectus Space (Similar to a Normal Retrorectus Ventral Hernia Repair)
- May Require a Transverse Abdominis Release (TAR) for Adequate Spacing
- Can Then Repair by Either a Sugarbaker or Keyhole Technique within This Space
- Mesh Kept Off the Bowel By this Approach
Sugarbaker is Preferred Over Keyhole Due to Lower Recurrence, But Otherwise No Significant Difference Between Onlay vs Intraperitoneal vs Sublay
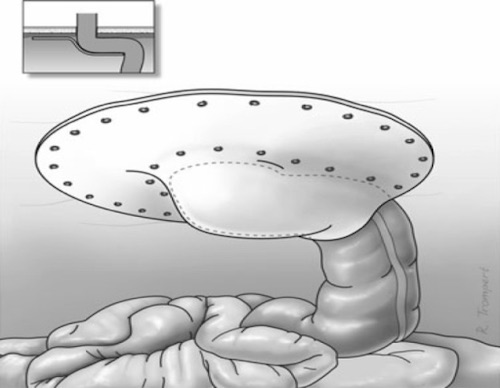
Sugarbaker Mesh Repair 2
References
- Haggstrom M. Wikimedia Commons. (License: CC BY-1.0)
- Hansson BM, Morales-Conde S, Mussack T, Valdes J, Muysoms FE, Bleichrodt RP. The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate: a multicenter cohort study. Surg Endosc. 2013 Feb;27(2):494-500. (License: CC BY-2.0)