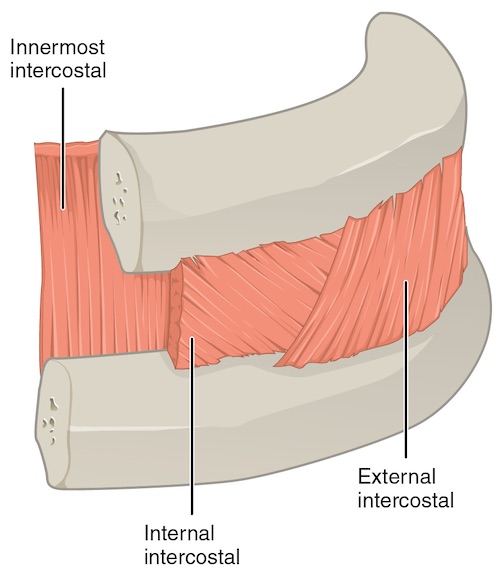
Lady of Hats. Wikimedia Commons. (License: Public Domain)
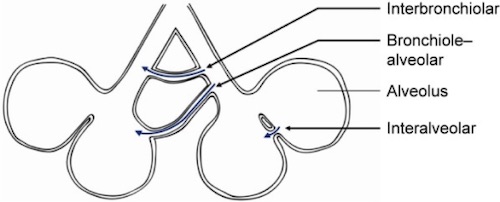
Koster TD, Slebos DJ. The fissure: interlobar collateral ventilation and implications for endoscopic therapy in emphysema. Int J Chron Obstruct Pulmon Dis. 2016 Apr 13;11:765-73.(License: CC BY-NC-3.0)