Chronic Constipation and a High-Fiber Diet is the Most Common Risk Factor – Lengthens the Intestine and Mesentery to Become Chronically Distended and Redundant
More Common in the 6th-8th Decade of Life (Compared to Cecal Volvulus Which is Most Common in the 4th-6th Decade of Life) – Due to Degenerative Colonic Disease Rather than Congenital Cecal Mobility
Highly Associated with Institutionalized Patients with Neuro-Psych Disorders
Neurologic Dysfunction
Dementia
Parkinson Disease
Multiple Sclerosis
Spinal Cord Injury
Psychiatric Disorders
Schizophrenia
Bipolar Disorder
Depression/Anxiety
Chronic Antipsychotic Use
Intellectual Disability/Developmental Delay
Long-Term Institutionalization
Risk Factors
Adhesions
Male Sex
More Common in African, Middle Eastern, and South American Populations
Laxative Abuse
Colonic Dysmotility
Immobility
Presentation and Diagnosis
Presentation
Abdominal Pain
Abdominal Distention
Nausea and Vomiting
Obstipation
May See an Explosive Bowel Movement if Spontaneously Detorses
Diagnosis
Generally Diagnosed by CT Abdomen/Pelvis
Sigmoid Colon is Dilated and Twisted
“Whirl Sign” with Mesentery Twisted
Abdominal Plain Film is More Sensitive (60-75%) than in Cecal Volvulus But is Still Generally Considered Poor at Diagnosis
Classic “Bent Inner-Tube Sign” (Dilated Loop of Colon with Apex in the Right Upper Quadrant) is Rarely Seen
Also Known as an “Omega Sign” or “Coffee-Bean Sign”
Suggestive Plain Film Findings Should Be Further Evaluated by CT
Can Be Diagnosed at Surgical Exploration in an Emergent Setting
Sigmoid Volvulus 2
Management
Hemodynamically Stable: Immediate Colonoscopic Decompression with Delayed Sigmoidectomy During the Index Admission
Endoscopic Detorsion:
Do Not Detorse and Proceed with Emergent Surgery if Any Signs of Ischemia or Perforation are Seen on Endoscopy
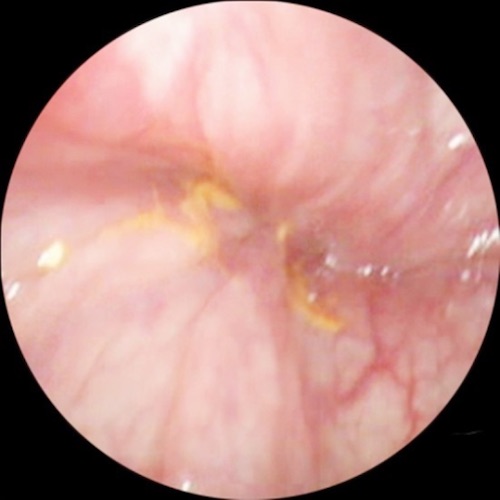
Mucosal Pinwheel/Spiral Seen at the Site of Obstruction Before Detorsion – Typically at the Rectosigmoid Junction
Insufflation and Gentle Pressure Can Untwist the Colon
Suction the Dilated Bowel of All Accumulated Gas and Stool to Decompress and Reduce
May See a Second Area of Spiral at the Point of Proximal Obstruction
Consider Leaving a Decompression Tube (Red Rubber Catheter or Rectal Tube) to Prevent Retorsion Prior to Surgery
Endoscopic Detorsion Outcomes:
80-95% Success Rate
40-75% Recur if Not Resected
Perform Surgical Resection During the Index Admission
Primary Anastomosis is Generally Preferred if Stable
Hemodynamically Unstable, Peritonitis, Ischemia/Necrosis, or Perforation: Emergent Resection
Hartmann Procedure with End Colostomy is Generally Preferred Over Primary Anastomosis
Sigmoid Volvulus Swirl on Sigmoidoscopy 3
References
Qadir I, Salick MM, Barakzai A, Zafar H. Isolated adult hypoganglionosis presenting as sigmoid volvulus: a case report. J Med Case Rep. 2011 Sep 8;5:445. (License: CC BY-2.0)
Elia F, Pagnozzi F, Busolli P, Aprà F. Frail patient with abdominal pain. West J Emerg Med. 2010 Sep;11(4):400-1. (License: CC BY-NC-4.0)
Atamanalp SS, Atamanalp RS. The role of sigmoidoscopy in thediagnosis and treatment of sigmoid volvulus. Pak J Med Sci. 2016 Jan-Feb;32(1):244-8. (License: CC BY-3.0)