Spontaneous Intestinal Perforation (SIP) in Newborns
Spontaneous Intestinal Perforation (SIP) in Newborns
James Myall, MD
Table of Contents
Definition
Definition: A Focal, Typically Solitary Bowel Perforation Occurring in Premature Neonates, Most Commonly Involving the Terminal Ileum
While classically described as a single perforation, rare cases of multiple focal perforations have been reported, though these remain uncommon and the disease is fundamentally characterized by localized, rather than diffuse, pathology.
Epidemiology and Risk Factors
SIP is Increasingly Recognized as a Leading Cause of Surgical Intestinal Disease in Extremely Low Birth Weight (ELBW) Infants
- Most Frequent in Infants Born at < 28 Weeks Gestation
- Peak Incidence in Those at 22-24 Weeks and in Infants Weighing < 1,500 g
Incidence: Ranges from 2-3% in Very Low Birth Weight (VLBW) Infants to as High as 10% in ELBW Populations, with Some Cohorts Demonstrating Rates Exceeding Those of Classical Surgical Necrotizing Enterocolitis (NEC)
Risk Factors
- Prematurity and Extreme Intestinal Immaturity
- Hemodynamic Instability and Vasopressor Requirement
- Exposure to Indomethacin or Other NSAIDs/COX Inhibitors
- Early Postnatal Corticosteroid Use
- Iatrogenic or Catheter-Related Interventions
Protective Factors
- Predominant Human Milk Feeding – Associated with Improved Intestinal Perfusion, Reduced Inflammation, and Enhanced Mucosal Integrity
- Early Advancement of Enteral Nutrition
- Minimization of Iatrogenic Stressors
Pathophysiology
SIP Results from Structural Intestinal Immaturity Compounded by Localized Ischemia and Impaired Tissue Repair, Rather Than Diffuse Inflammatory Necrosis
In Premature Neonates, the Intestinal Wall is Underdeveloped (Particularly in the Terminal Ileum)
- Reduced Muscular Integrity
- Immature Microvasculature
- Limited Reparative Capacity
Superimposed Localized Hypoperfusion Leads to Focal Ischemic Injury (Often in Watershed Regions of Mesenteric Circulation)
This Explains Why SIP Produces a Single Focal Perforation Rather Than Diffuse Disease
- Watershed Perfusion Zones Predispose to Localized Ischemia
- Transient Hypoperfusion Events (Hypotension, Vasopressors, etc.) Create Discrete Injury
- Intrinsic Wall Weakness in Immature Bowel Limits the Ability to Withstand Localized Stress
Medication Exposures Further Contribute
- Indomethacin (COX Inhibition) Reduces Prostaglandin Synthesis – Causes Vasoconstriction, Decreased Mesenteric Blood Flow, and Exacerbates Ischemia
- Corticosteroids Impair Collagen Synthesis and Mucosal Repair – Weakens the Intestinal Wall and Limits Healing Capacity
Together, These Factors Result in Focal Bowel Wall Failure Without the Widespread Inflammation and Necrosis Characteristic of NEC
Clinical Presentation and Diagnosis
SIP Is Diagnosed Through a Combination of Clinical Presentation and Imaging, with Surgical Findings Providing Definitive Diagnosis
Typically Presents Within the First Week of Life – Often Earlier Than NEC (Which More Commonly Develops After the First to Several Weeks of Life)
Clinical Presentation
- Abrupt Abdominal Distension
- Abdominal Discoloration or Erythema
- Increased Ventilatory Requirements
- Metabolic Acidosis
- Hemodynamic Instability or Shock
- Decreased Bowel Sounds
Radiographic Findings
- Pneumoperitoneum (Most Common and Often Diagnostic)
- Isolated Bowel Loop Dilation
- Gasless Abdomen in Severe Cases
- Relative Absence of:
- Pneumatosis Intestinalis
- Portal Venous Gas
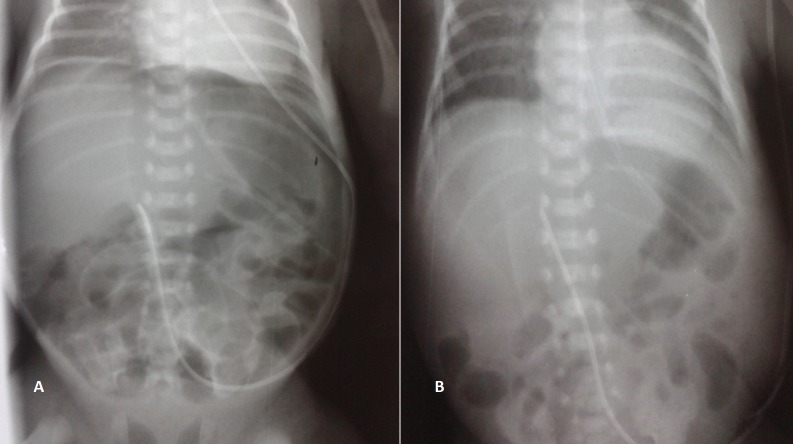
Pneumoperitoneum (A), Resolution After Peritoneal Needle Suction (B) 1
Differentiation from Necrotizing Enterocolitis (NEC)
Distinguishing SIP From NEC Is Critical, as Management and Prognosis Differ
| Feature | SIP | NEC |
| Timing | First Week of Life | Typically After First Week |
| Pathology | Focal Perforation | Diffuse Inflammation/Necrosis |
| Imaging | Pneumoperitoneum, No Pneumatosis | Pneumatosis, Portal Venous Gas |
| Distribution | Localized | Multifocal |
Management
Definitive Management is Surgical and Typically Involves Exploratory Laparotomy with Control of the Perforation After Resuscitation and Physiologic Optimization
Initial Stabilization
- Airway and Ventilatory Support
- Fluid Resuscitation and Correction of Electrolyte Abnormalities
- Broad-Spectrum Antibiotics
- Gastric Decompression via Nasogastric Tube – Reduces Intestinal Distension and Minimizes Further Compromise
- Consider Needle Decompression or Peritoneal Drainage (PD) in Cases of Abdominal Compartment Syndrome – Relieves Intra-Abdominal Pressure and Improves Ventilation and Perfusion
Peritoneal Drainage (PD)
- Peritoneal Drainage is a Bedside Procedure Typically Performed in Unstable Neonates Who Are Not Immediate Candidates for Laparotomy
- Techniques:
- Open Incisional Drainage – A Small Incision is Made on the Abdomen (Usually Right Lower Quadrant) and Carried Down Through the Fascia to Place a Drain into the Peritoneal Cavity (Penrose or Silicone/JP Drain)
- Percutaneous Drainage – Classic Seldinger Technique Using a Hollow Bore Needle, Guidewire, and Pigtail Catheter
- Purpose:
- Decompression of Pneumoperitoneum
- Drainage of Contaminated Peritoneal Fluid
- Temporary Stabilization Prior to Definitive Surgery
- In Select Cases, PD May Serve as Definitive Management, Though This Remains Debated
Definitive Surgical Management (Exploratory Laparotomy):
- Direct Inspection of Bowel
- Primary Repair or Segmental Resection
- Creation of Ostomy if Indicated
Outcomes
Survival
- SIP: 70-90% in ELBW Infants
- Surgical NEC: 50-70%
Morbidity
- Reoperation
- Stoma Formation
- Prolonged Parenteral Nutrition
- Sepsis
- Long-Term Growth and Neurodevelopmental Impairment
Poor Prognostic Factors
- Lower Gestational Age
- Hemodynamic Instability at Presentation
- Delay in Surgical Intervention
References
- Chioukh FZ, Ben Ameur K, Laamiri R, Ben Hmida H, Nouri A, Monastiri K. Spontaneous Intestinal Perforation in a Very Low Birth Weight Infant: Successful Management by Peritoneal Needle Suction. J Neonatal Surg. 2016 Jul 3;5(3):39. (License: CC BY-3.0)