
Cervical Collar 1
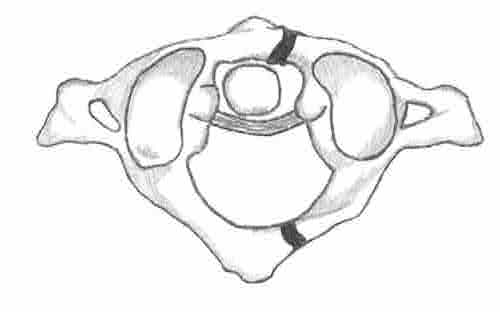
Jefferson Fracture

Jefferson Fracture
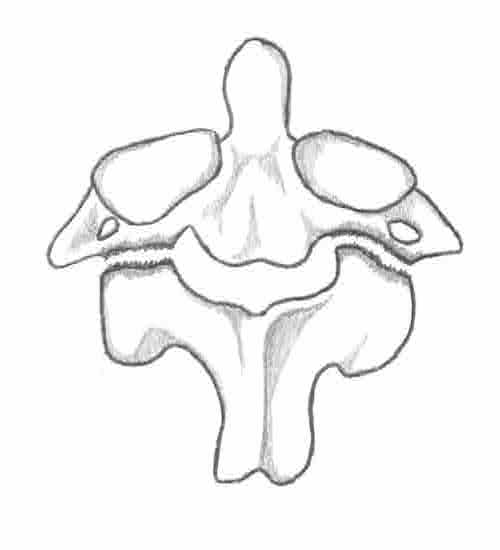
Hangman’s Fracture
Hangman’s Fracture
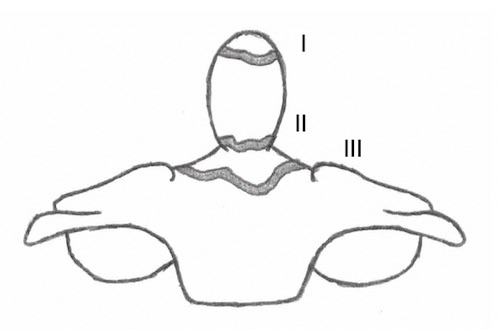
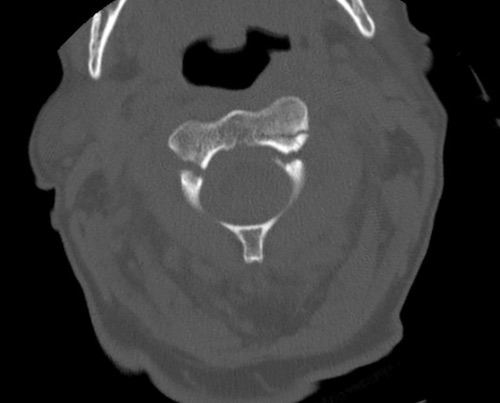
C2 Dens Fracture, Types

C2 Dens Fracture
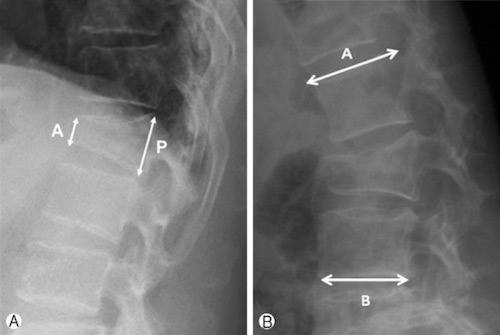
Wedge Fracture 2

Burst Fracture 3
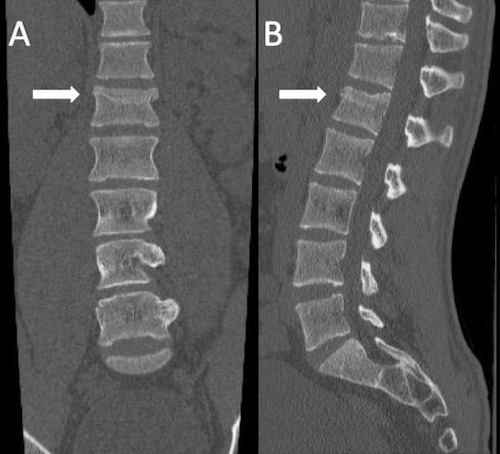
Chance Fracture 4
![]()
Transverse Process Fracture 5

Spinous Process Fracture 6
Cervical Collar 1
Jefferson Fracture
Jefferson Fracture
Hangman’s Fracture
Hangman’s Fracture
C2 Dens Fracture, Types
C2 Dens Fracture
Wedge Fracture 2
Burst Fracture 3
Chance Fracture 4
![]()
Transverse Process Fracture 5
Spinous Process Fracture 6