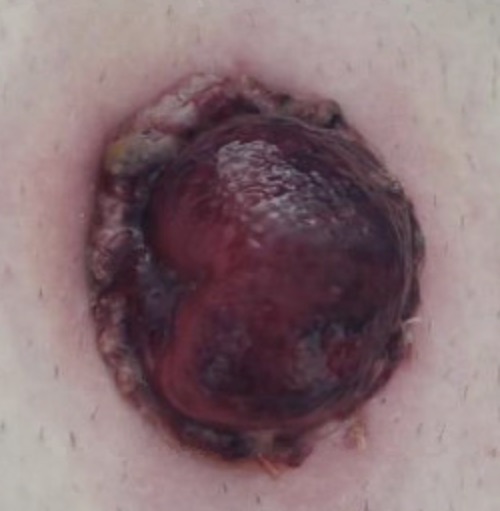
Stomal Ischemia/Necrosis Stomal Ischemia/Necrosis David Ray Velez, MD Table of Contents DefinitionsRisk FactorsManagementSee Also:*See Ostomy Definitions Stomal Ischemia/Necrosis: Inadequate Blood Supply (Ischemia) of the Stoma that Can Cause Tissue Death (Necrosis)Causes a Dusky/Dark AppearanceIncidence: 2-16%Venous CongestionStomas Can Frequently Appear “Dusky” Shortly After Surgery without Overt Arterial CompromiseSwelling and Constriction Causes Venous CongestionVenous Congestion Causes Further Swelling and Cyanosis (Appearing Ischemic)Normal Color Returns Once Postoperative Edema Resolves and Venous Outflow Improves*Caution: Venous Congestion Can Progress with Worsening Swelling that Eventually Causes Ischemia with Impairment of Arterial Inflow Stomal Ischemia Stomal Necrosis Risk Factors Patient FactorsObesityIBDVascular DiseaseDiabetesSurgical FactorsTensionDevascularization/Inadequate Blood Supply to the ConduitInadequate Size of Fascial/Skin OpeningColostomy – Worse Blood Supply than the Small BowelEnd Ostomy – Loop Ostomies Have a Dual Blood Supply from Both the Proximal and Distal LimbsEmergency Surgery Management The First Step Must Be to Evaluate the Extent of Necrosis (Determine if it Extends Above or Below the Level of the Fascia)Test-Tube Evaluation: A Lubricated Test Tube Inserted into the Stoma and a Flashlight is Directed Through to Evaluate the Surrounding MucosaEndoscopic Evaluation: Anoscope or Flexible Sigmoidoscopy Inserted into the StomaSuperficial (Distal) to Fascia: Observe and Monitor ProgressionCan Progress and Extend Past the Fascia Eventually Requiring Surgical RevisionCan Cause Mucocutaneous Separation or Stomal Stenosis/Stricture as it HealsExtends Beyond (Proximal to) Fascia: Immediate Surgical RevisionGenerally Requires Laparotomy with Ostomy RevisionRisk for Necrosis with Potential Stool Spillage if Not Revised