Short (< 7-10 cm): Heineke-Mikulicz Stricturoplasty
Intermediate (> 7-10 cm): Finney Stricturoplasty
Long (> 15-20 cm): Michelassi Stricturoplasty
Principals
Always Inspect Mucosa to Rule Out Underlying Malignancy & Bx Any Suspicious Lesions
Ensure Hemostasis
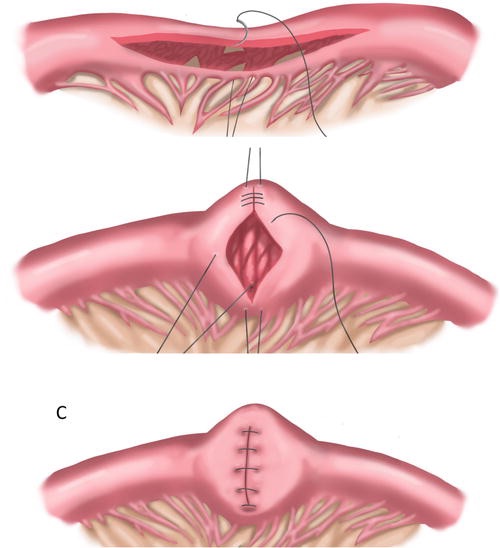
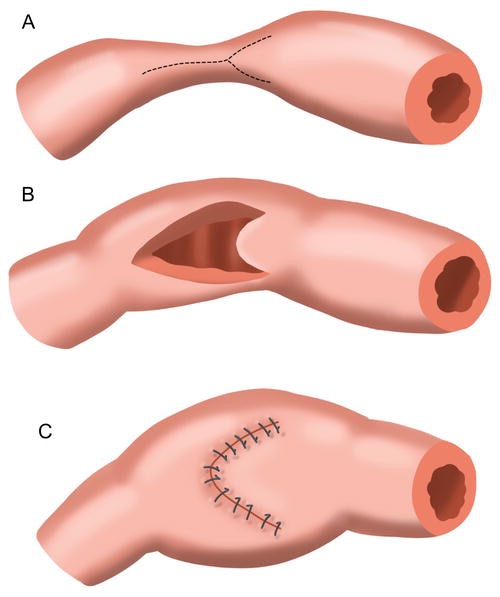
Heineke-Mikulicz Stricturoplasty
Most Common Approach
For Small (< 7-10 cm) Strictures
Procedure:
Isolate the Diseased Segment
Make a Longitudinal Incision Along the Antimesenteric Border
Extend 2 cm Proximal & Distal to the Structured Area
Close the Incision Transversely
Use Traction Sutures at the Midpoints to Pull and Assist in Closure
Close in 1-2 Layers
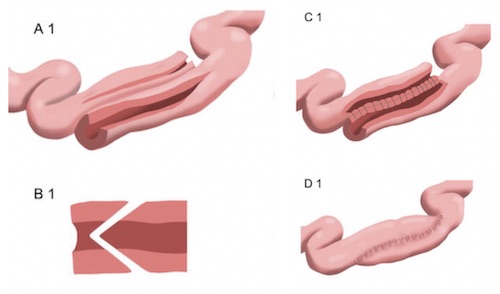
Finney Stricturoplasty
For Intermediate (> 7-10 cm) Strictures
Procedure:
Isolate the Diseased Segment
Diseased Segment is Folded onto Itself at the Midpoint
Make an Extended “U-Shaped” Incision Along the Antimesenteric Border
Extend 2 cm Proximal & Distal to the Structured Area
Closed Side-to-Side
Start at the Middle
Suture Inferior Leaf of the Proximal Half to the Inferior Leaf of the Distal half
Continue to Suture the Superior Leaves
Finish with a Layer of Lembert Sutures to Invert
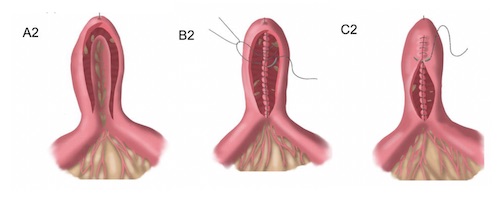
Michelassi Stricturoplasty
For Large (> 15-20 cm) Strictures
Procedure:
Isolate the Diseased Segment
Transect Diseased Segment at the Midpoint
Transfer the Proximal Limb Next to the Distal Limb
Lay in an Isoperistaltic Side-to-Side Manner
Place a Posterior-Row of Nonabsorbable Suture to Approximate
Make Longitudinal Incisions Over the Approximated Sides to Spatulate
Close Internal Layers with a Running Absorbable Suture
Oversew the Anterior Layer with Nonabsorbable Suture
Other Stricturoplasty Options
Jaboulay Stricturoplasty
Side-to-Side Anastomosis Bypassing the Strictured Segment
Use: If Stricture is Too Tight or Unable to Suture
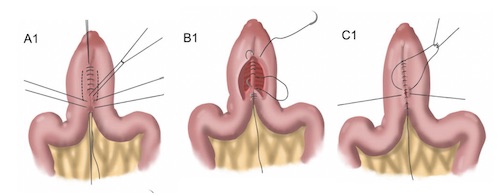
Moskel-Walske-Neumayer Stricturoplasty
“Y” Incision Closed Transversely
V Portion in Dilated Bowel
Use: If Stricture Short with Significant Size Difference Between Proximal & Distal Segments
Complications
Most Common: Bleeding
Anastomotic Leak
Dehiscence
SBO
Heineke-Mikulicz 1
Finney 1
Michelassi 1
Jaboulay 1
Moskel-Walske-Neumayer 1
References
Oliveira EC, Bafutto M, Bafutto AAF, Neto SG, Neto JJB. Current Elective Surgical Treatment of Inflammatory Bowel Disease. Current Topics in Colorectal Surgery, IntechOpen, 2021. (License: CC BY-3.0)