Cholelithiasis (Gallstones)
Cholelithiasis (Gallstones)
Richard Knight, MD
Table of Contents
Definitions
Cholelithiasis (Gallstones): Calculi/Stones Found within the Biliary System
Subtypes Based on Location:
- Cholecystolithiasis: Calculi/Stones Found within the Gallbladder
- Choledocholithiasis: Calculi/Stones Found within the Bile Ducts
*Cholelithiasis and Cholecystolithiasis are Often Used Interchangeably Although Technically Cholelithiasis is a Broader Term that Encompasses Both Cholecystolithiasis and Choledocholithiasis
Overall Gallstone Prevalence in General Population: 7-20%
Types of Stones
Classification
- Nonpigmented Stones
- Cholesterol Stones
- Pigmented Stones
- Black Stones
- Brown Stones
- Mixed Stones – Contain Both Pigmented and Nonpigmented Components
Nonpigmented/Cholesterol Stones are the Most Common (80%) in the United States, but Pigmented Stones are the Most Common in the World
Cholesterol Stones
- Composed of Cholesterol
- The Only Nonpigmented Stone
- Causes:
- Stasis
- Increased Water Resorption
- Low Lecithin Ratio
- Low Bile Salts
- High Cholesterol
- Risk Factors:
- Female
- Elderly
- Pregnancy
- Obesity
- Rapid Weight Loss – Common After Gastric Bypass
- Diabetes
- Hispanic or Native American
Black Stones
- Composed of Calcium Bilirubinate
- Excess Unconjugated Bilirubin Interacts with Calcium to Form Calcium Bilirubinate
- Caused by Hemolysis or Excess Bilirubin
- Associated With:
- Total Parenteral Nutrition (TPN)
- Cirrhosis
- Alcoholism
- Biliary Tract Infection
- Chronic Hemolysis
- Pancreatitis
- Advanced Age
Brown Stones
- Composed of Insoluble Calcium Salts
- Infected Bile Enhances Hydrolytic Enzymes (Beta Glucuronidase, Phosphorolipase A, and Conjugated Bile Acid Hydrolase)
- Hydrolysis of Bilirubin Forms Insoluble Calcium Salts
- Stones are Found Within Both the Gallbladder and Bile Ducts
- The Predominant de Novo Bile Duct Stone (Cholangiohepatitis)
- Most Common in Asians
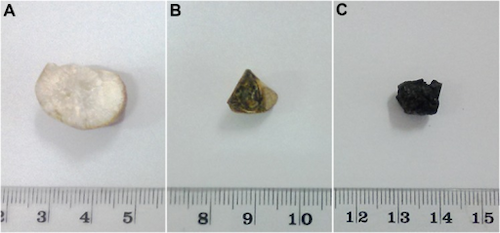
(A) Cholesterol Stone, (B) Mixed Stone, (C) Black Stone 1
MNEMONIC: Risk Factors for Gallstones
4 F’s: “Fat Fertile Female in Her Forties”
*Some Say “5 F’s” Including “Fair” – However, This is Based on the Misconception that Gallstones are Most Common in Caucasians When in Actuality they are More Common in Hispanics and Native Americans
Presentation
Symptoms are Caused by Intermittent Cystic Duct Obstruction by the Gallstones
Abdominal Pain
- Intense Dull Right Upper Quadrant (RUQ) Pain
- Lasts 30 Minutes-6 Hours
- Worse After Fatty Meal, Triggering Gallbladder Contraction
- Usually Constant and Not “Colicky”
The Term “Biliary Colic” is Occasionally Used to Describe Symptomatic Cholelithiasis Although it is a Misnomer – Pain is Constant for Several Hours (Does Not Wax/Wane)
Additional Symptoms
- Nausea
- Vomiting
- Other Symptoms Such as Fever, Chills, Jaundice, Clay-Colored Stools, and Dark Urine are Concerning for Other Complications
Hydrops Gallbladder
- Describes Mucus Distention of the Gallbladder
- Caused by an Impacted Stone Without Associated Infection
- Over Time Bile is Absorbed and Mucus is Secreted
- Hydrops Alone Can Create a Palpable but Nontender Gallbladder
- No Increased Risk of Malignancy
Complications
- Cholecystitis – *See Cholecystitis
- Cholangitis – *See Cholangitis
- Gallstone Pancreatitis – *See Acute Pancreatitis
- Gallstone Ileus – *See Gallstone Ileus
- Gallstone Cancer – *See Gallbladder Adenocarcinoma
Most Often Remain Asymptomatic or Develop Symptoms Before the Development of Complications
Diagnosis
Ultrasound is the Preferred Diagnostic Test
May Also Be on Other Imaging (CT/MRI)
Consider MRCP/ERCP if Concerned for Choledocholithiasis
Labs (CBC/CMP) are Not Specific for Cholecystolithiasis but May Be Indicated if Concerned for Choledocholithiasis or Associated Complications

Large Gallstone Seen on US 2
Treatment
Asymptomatic Cholelithiasis: Nothing
- Asymptomatic Cholelithiasis is a Benign and Common Finding that Generally Does Not Require Any Specific Intervention
Symptomatic Cholelithiasis: Elective Cholecystectomy
Ursodeoxycholic Acid (UDCA/Ursodiol)
- Rarely Used in Modern Practice but May Trial for Medical Management of Symptomatic Cholelithiasis if Patient Refuses Surgery
- Dissolution Therapy
- Only Considered for Small Stones (< 1 cm) that are Symptomatic with a Functioning Gallbladder
- 40% Success but 50% Recurrence in 5 Years if Therapy is Stopped
Indications for Prophylactic Cholecystectomy with Asymptomatic Cholelithiasis
- Large Stones (> 3 cm) – Risk for Malignancy
- Pediatrics – Unreliable History
- Liver Transplant
- Sickle Cell Disease – Episodes Can Mimic a Sickle Cell Crisis
- Hereditary Spherocytosis (If Already Preforming Splenectomy)
- Controversial Indications:
- Concomitant with Gastric Bypass
- Increased Risk of Gallstones but They are Generally Asymptomatic
- Not Indicated if No Gallstones Are Found
- Stronger Indication if Concomitant with a Duodenal Switch
- Spinal Cord Trauma
- Some Consider a Relative Indication
- Symptoms Not Necessarily Obscured by Injury
- Concomitant with Gastric Bypass
References
- Weerakoon H, Navaratne A, Ranasinghe S, Sivakanesan R, Galketiya KB, Rosairo S. Chemical characterization of gallstones: an approach to explore the aetiopathogenesis of gallstone disease in Sri Lanka. PLoS One. 2015 Apr 8;10(4):e0121537. (License: CC BY-4.0)
- Nevit Dilmen. Wikimedia Commons (License: CC BY-SA-3.0)