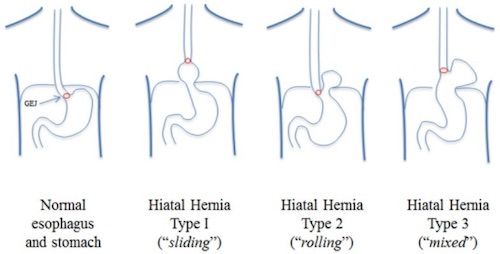
Hiatal Hernia Types 1

Esophagram – Sliding HH 2
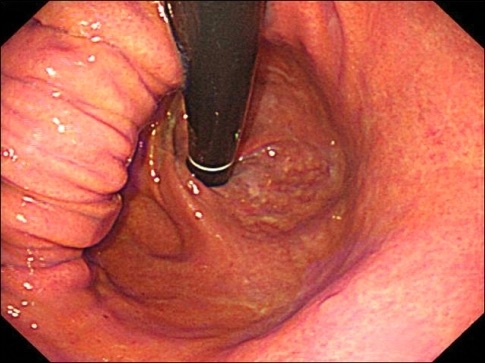
Endoscopy – Sliding HH 2
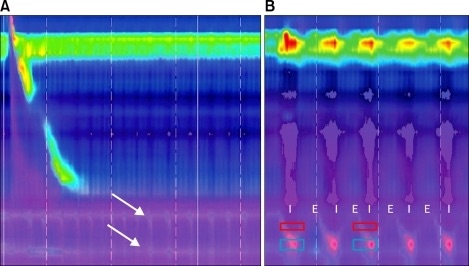
Manometry – Hypotensive Contraction 2
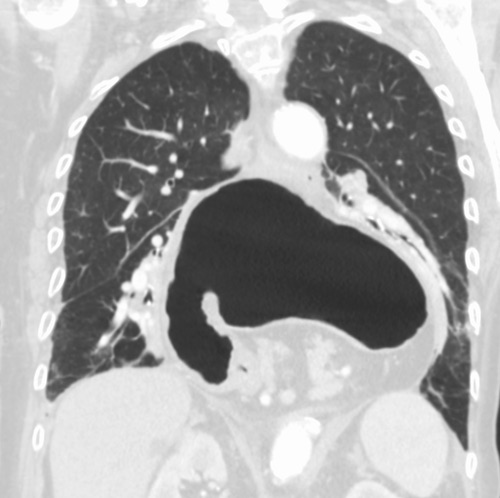
CT Showing Large Type IV HH 3
Hiatal Hernia Types 1
Esophagram – Sliding HH 2
Endoscopy – Sliding HH 2
Manometry – Hypotensive Contraction 2
CT Showing Large Type IV HH 3