Subtotal Cholecystectomy: Removal of Almost All of the Gallbladder
Partial Cholecystectomy: Removal of Only Part of the Gallbladder
Quantitively Less Than a Subtotal Cholecystectomy Although Often Used Interchangeably
Fundectomy: Removal of Only the Top-Half or Less of the Gallbladder
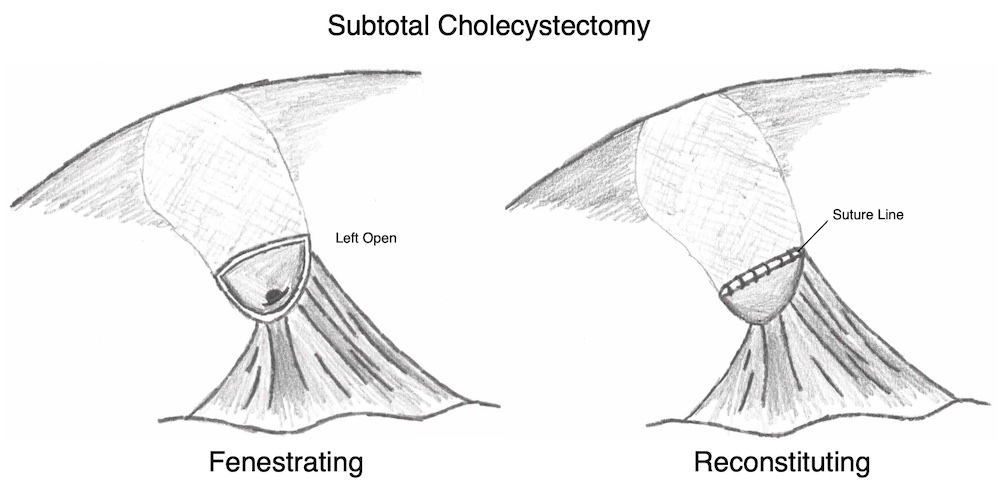
Types of Subtotal Cholecystectomy
Subtotal Fenestrating Cholecystectomy: Leaves the Lumen Open and Does Not Produce a Remnant Gallbladder
Generally the Preferred Technique in These Situations
Subtotal Reconstituting Cholecystectomy: Closes the Lumen to Produce a Small Remnant Gallbladder
Outcomes
Subtotal Fenestrating Cholecystectomy
Higher Risk of Bile Leak (14.1% vs 7.9%) – 20% Resole Spontaneously and 75% Resolve with ERCP
Subtotal Reconstituting Cholecystectomy
Higher Risk for Recurrent Stones or Remnant Cholecystitis (11.6% vs 3.1%)
No Difference in Bile Duct Injury, Infection, Re-Operation, or Need for Completion Cholecystectomy
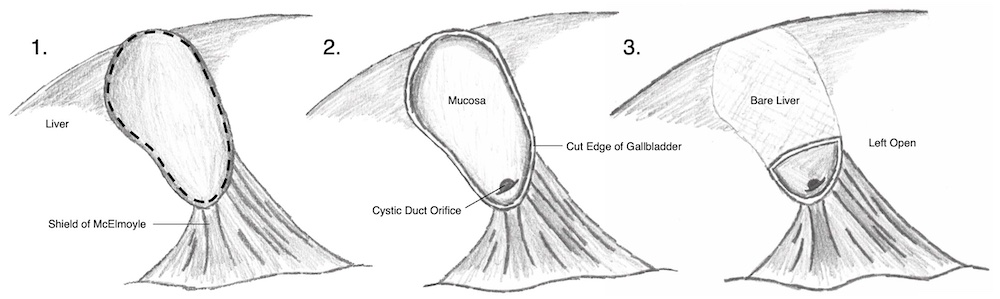
Fenestrating Technique
Generally Start by Attempting a Routine Cholecystectomy and Then Transition to a Subtotal Cholecystectomy as a “Bail Out” Once Approaching a Zone of Significant Risk
*Gallbladder May Already Be Perforated and Inadvertently Opened During a Difficult Dissection
Bile, Stones, and Debris are Suctioned or Removed
Safety Landmarks
The Cystic Duct/Artery are Not Dissected
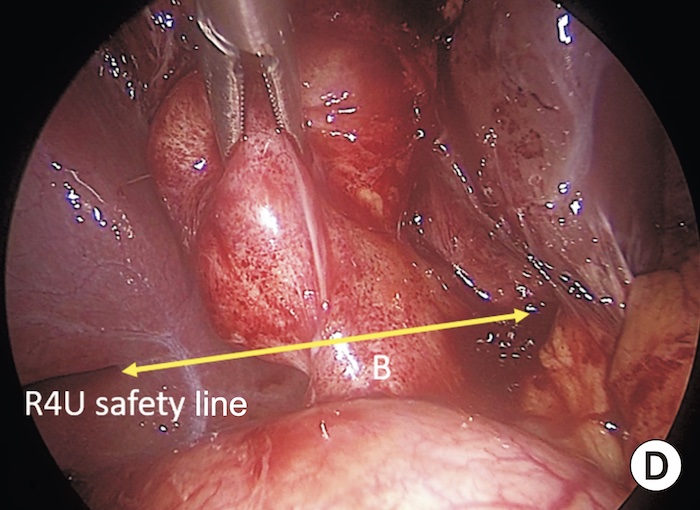
“Line of Safety” – An Imaginary Line Extending from Rouviere’s Sulcus to the Base of Segment 4b
All Dissection Should Remain Superior to This “Line of Safety”
“Shield of McElmoyle” – Refers to the Peritoneum Overlying the Cystohepatic Triangle
The Bottom Lip of the Free Peritonealized Gallbladder is Left Behind to Protect from Entering the Hepatocytic Triangle
Remove the Gallbladder*
The Gallbladder Incision is Extended Posteriorly Around the Gallbladder Neck
The Anterior Wall of The Gallbladder is Completely Removed
The Posterior Wall is Generally Left on the Cystic Plate Although the Superior-Most Portion May Be Excised
Remnant Mucosa is Ablated by Cautery or Argon Beam
Completion
May Consider Purse-String Closure of the Cystic Duct from the Inside if Feasible – Often Foregone Due to Safety Concerns
Leave a Drain Near the Stump to Drain the Presumed Bile Leak (3x Risk)
Close the Port Sites or Laparotomy Incision
Fenestrating Subtotal Cholecystectomy
Line of Safety Above a Retracted CBD (B) 1
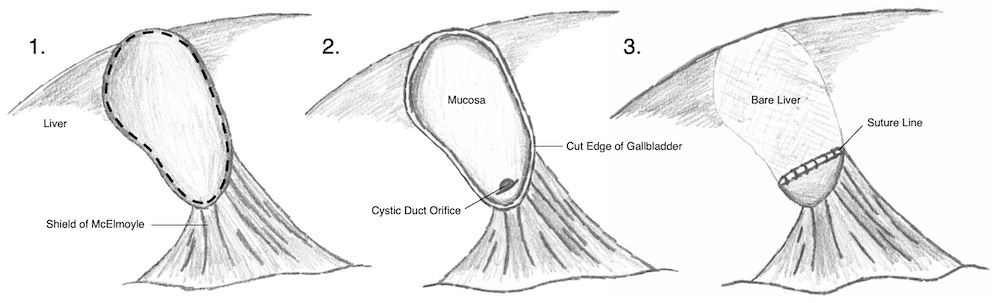
Reconstituting Technique
Generally Start by Attempting a Routine Cholecystectomy and Then Transition to a Subtotal Cholecystectomy as a “Bail Out” Once Approaching a Zone of Significant Risk
The Procedure is Similar to a Fenestrating Technique
Instead of Leaving Open, The Lumen is Closed with Sutures or Staplers
Reconstituting Subtotal Cholecystectomy
References
Gupta V. How to achieve the critical view of safety for safe laparoscopic cholecystectomy: Technical aspects. Ann Hepatobiliary Pancreat Surg. 2023 May 31;27(2):201-210. (Liscence: CC BY-NC-4.0)