Ventral Hernia
Ventral Hernia
David Ray Velez, MD
Table of Contents
Definitions and Descriptors
Definitions
- Ventral Hernia: Hernia of the Anterior Abdominal Wall
- Types:
- Incisional Hernia: Hernia Through a Prior Incision
- Umbilical/Periumbilical Hernia: Hernia Through the Umbilical Ring
- Epigastric Hernia: Hernia Between the Umbilicus and Xiphoid Along the Linea Alba
- Spigelian Hernia: Hernia Along the Spigelian Line (Aponeurotic Band at Lateral Border of the Rectus Abdominis)
- Arcuate Line Hernia: Hernia Through the Arcuate Line
- Posterior Rectus Sheath Hernia: Hernia Through the Posterior Rectus Sheath
- Rectus Abdominis Diastasis: Separation of Rectus Abdominis Pillars
- Fascia Intact (Not a True Hernia)
- *See Rectus Abdominis Diastasis (RAD)
- Reducible: Able to Reduce/Push the Hernia Contents Back into the Abdominal Cavity
- Incarcerated: Unable to Reduce/Push the Hernia Contents Back into the Abdominal Cavity
- Causes a Risk of Strangulation
- Strangulated: Hernia Blood Supply is Obstructed
- Causes a Risk of Ischemia and Necrosis (Surgical Emergency)
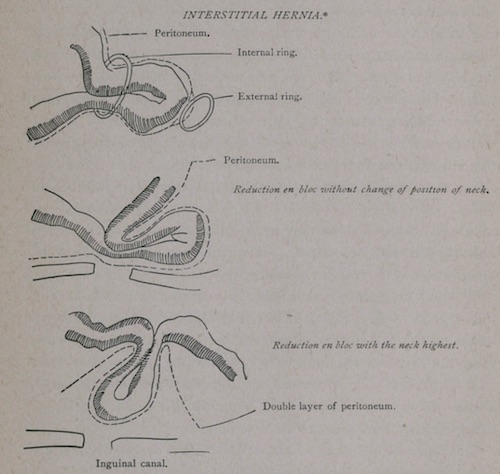
- Reduction en Masse: Hernia Sac is Reduced but the Bowel is Still Incarcerated within the Reduced Sac 1
- Causes a Risk of Progression to Ischemia and Necrosis Despite Reduction
- “Classically” Describing an Inguinal Hernia 1
- Richter Hernia: Only the Antimesenteric Border of the Bowel Wall is Herniated 2
- Also Described as a “Partial Enterocele” 2
- May Not Cause Obstruction as Bowel Contents Can Pass Through the Intraperitoneal Portion of the Bowel
- High Risk of Incarceration and Strangulation of the Herniated Portion
- Interparietal Hernia: Hernia Between the Layers of the Anterior Abdominal Wall 3
- Most Commonly Due to an Incisional Hernia
- Littre Hernia: Hernia Contains a Meckel Diverticulum 4
- Amyand Hernia: Hernia Contains the Appendix 5
- “Classically” Describing an Inguinal Hernia
- Sliding Hernia: A Retroperitoneal Organ is Included as Part of the Hernia Sac 6
- Most Common Organs:
- Males: Sigmoid Colon and Cecum
- Females: Ovary and Fallopian Tube (Ligate the Round Ligament and Return the Ovary at Surgery)
- Most Common Organs:
- Small: < 1 cm
- Medium: 1-4 cm
- Large: > 4 cm

Large Ventral Hernia 8
Reduction en Masse 1
Richter Hernia 9
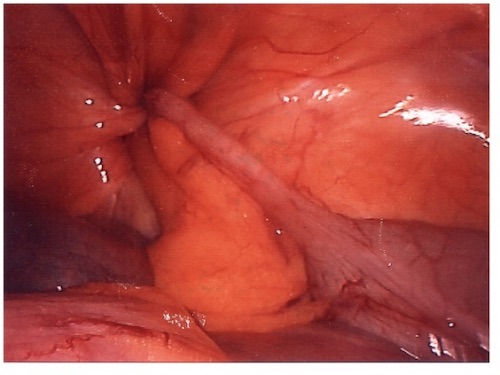
Amyand Hernia 10
Types of Hernias
Incisional Hernia
- Definition: Hernia Through a Prior Incision
- Port-Site Hernia: Incisional Hernia Through a Prior Port Site
- Develop in 10-15% of Incisions 11
- Highest for Midline Incisions (3-20%) 12,13
- Pfannenstiel Incisions are Significantly Lower Risk (0-2%) 14
Umbilical/Periumbilical Hernia
- Definition: Hernia Through the Umbilical Ring
- More Common in Women (3:1 Ratio)
- Incidence Among Pregnancies: 0.08% 15
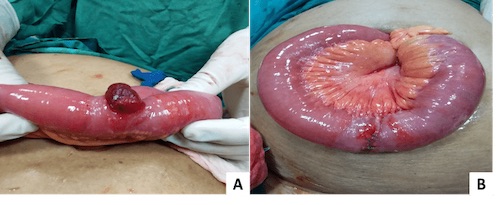
- Proboscoid (Elephant-Trunk) Hernia 16
- Definition: A Large Umbilical Hernia with Excessive Stretching of the Skin Resembling a Trunk
- Named After the Nose of a Proboscis Monkey
- Usually At Least a Few cm in Diameter

Umbilical Hernia 22

Proboscoid Hernia 23
Epigastric Hernia
- Definition: Hernia Between the Umbilicus and Xiphoid Along the Linea Alba
- Due to a Weakened Linea Alba 17
- Congenitally from Lack of Decussating Fibers
- Forceful Diaphragmatic Contractions Transmitted to the Abdominal Wall
- Perforation by Vascular Lacunae
- Ventral Hernias are More Common Above the Umbilicus Than Below
- Obliterated Umbilical Vessels & Urachus Reinforce Abdominal Wall Below
- Up to 20% Have Multiple Defects
Spigelian Hernia
- Definition: Hernia Along the Spigelian Line (Aponeurotic Band at Lateral Border of the Rectus Abdominis)
- Most are Interparietal Between the Internal and External Obliques
- The Spigelian Line is Composed of Fibers from the Internal Oblique and Transversus Abdominis Aponeuroses
- Most Common at the Junction of the Arcuate Line
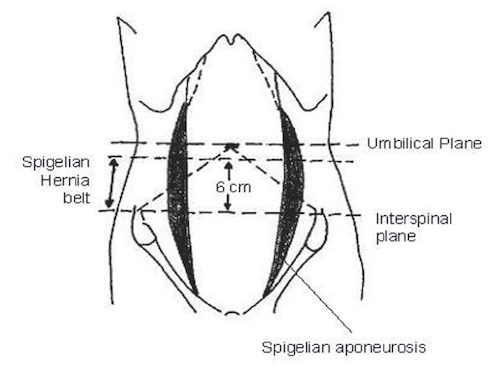
- “Spigelian Hernia Belt” – Horizontal Area Across the Abdominal Wall Bounded by the Interspinous Plane Inferiorly and 6 cm Above 18
- Interspinous Plane – Transverse Plane Between the Anterior Superior Iliac Spines
- Due to Variable Position of the Arcuate Line
- Contains 85-90% of Spigelian Hernias 18
- Often Difficult to Palpate and Can Be Confused with a Rectus Sheath Hematoma – Generally Require Imaging for Diagnosis
- Tend to Be Small with a Narrow Neck and High Risk of Incarceration/Strangulation

Spigelian Hernia 24
Spigelian Hernia Belt 18
Arcuate Line Hernia
- Definition: Hernia Through the Arcuate Line 19
- Hernia Sac Ascends Upward Between the Posterior Aponeurotic Sheath and Rectus Abdominis Muscle
- Defined as an Interparietal Hernia Within the Layers of the Abdominal Wall
- Can Be Unilateral or Bilateral 20
- The Majority are Asymptomatic Due to a Wide Hernia Orifice 19
- Often Misdiagnosed as a Spigelian Hernia
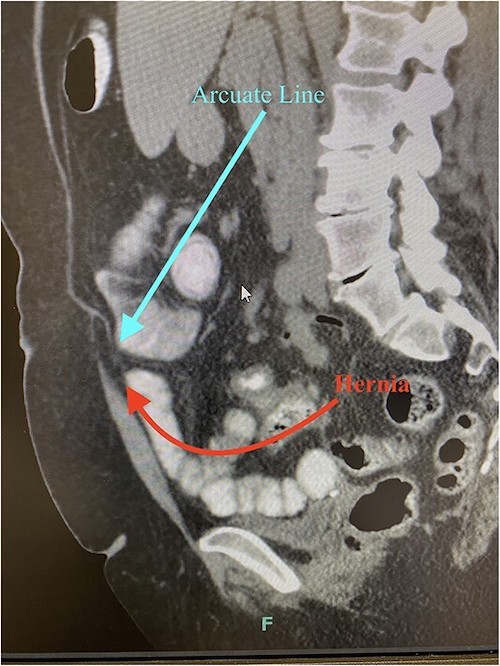
Arcuate Line Hernia on CT 19
Posterior Rectus Sheath Hernia
- Definition: Hernia Only Through the Posterior Rectus Sheath 21
- Defined as an Interparietal Hernia Within the Layers of the Abdominal Wall
- Presents as a Mass Within the Rectus Muscle (Can Be Confused with a Rectus Sheath Hematoma)
Risk Factors
General Ventral Hernia Risk Factors 17,25
- Extensive Physical Training
- History of Lifting or Pushing Heavy Objects (May Be Related to Occupation)
- Straining During Bowel Movements
- Coughing/Lung Disease
- Severe Vomiting
- Obesity
- Diabetes
- Smoking
- Steroid Use
- Older Age
- Male Sex (Umbilical Are More Common in Females)
- Pregnancy
Incisional Hernia Risk Factors 26,27
- Patient Factors:
- Obesity – Possibly the Most Important Patient Factor
- Malnutrition
- Older Age
- COPD
- Diabetes
- Smoking
- Immunosuppression
- Cystic Fibrosis
- Connective Tissue Disorders
- Technical Factors:
- Surgical Site Infection (Risk of Hernia Up to 25%)
- Suboptimal Fascial Closure
- Vertical Midline Incisions (Compared to Transverse or Oblique Incisions)
Presentation and Diagnosis
Presentation
- Abdominal Wall Bulge
- Abdominal Pain and Discomfort
- May be Worsened by Coughing or Straining
- Symptoms of Bowel Obstruction
- Nausea and Vomiting
- Constipation
- Overlying Skin Can Develop Erythema, Ischemia, or Ulceration Due to Excessive Pressure
Diagnosis
- Generally a Clinical Diagnosis
- Small Hernias May Be Difficult to Palpate
- Imaging May Be Required if Uncertain
- US – More Cost Effective and Allows Dynamic Assessment with Valsalva (Operator Dependent)
- CT – Allows Better Evaluation of Large and Complex Defects
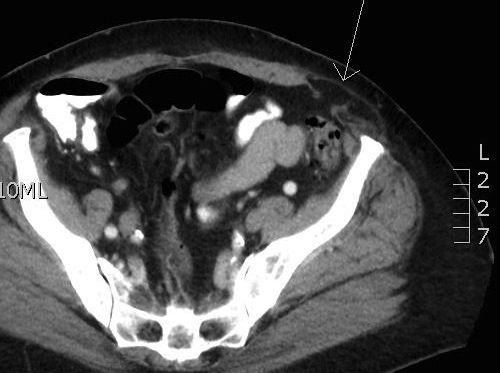
Spigelian Hernia on CT 28
Treatment
General Treatment 7,29
- Asymptomatic: Observe
- Consider Repair for Asymptomatic Patients Based on Patient Preference
- All Spigelian Hernias Should be Repaired Due to Risk of Incarceration/Strangulation
- Symptomatic: Surgical Repair
- *See Ventral Hernia Repair (VHR)
- Acutely Incarcerated or Strangulated Hernias Require Emergent Repair
- Chronically Incarcerated Hernias Can Be Managed by Observation or Elective Repair
- Mesh Indications: ≥ 1-2 cm (In General, if a Mesh Can Fit Through the Defect it Should be Used)
Management in Acute Care 30
- Indications for Emergent Surgery:
- Signs of Strangulation:
- Obstruction with Severe Pain
- Hypotension/Tachycardia
- Elevated Lactate and WBC
- Erythema or Bruising/Discoloration Over the Hernia
- Peritonitis
- Signs of Strangulation:
- Indications for Urgent Surgery (Same Admission):
- Acutely Incarcerated/Not Reducible
- Persistent Pain After Reduction
- Imaging Concerning for Strangulation:
- Fluid in the Hernia Sac
- Transition Point at the Neck of the Hernia
- Bowel Thickening in the Hernia
- Inflammatory Stranding Around the Hernia
- Consider Same Admission Surgery After Shared Decision Making if Poor Access to Outpatient Follow Up or High Risk of Recurrence (Ex: Femoral, Spigelian, Female Groin Hernia, Narrow Fascial Defect Compared to Hernia Size, Rapid Escalation of Symptoms, or Need for Conscious Sedation to Reduce)
Surgical Repair in the Obese 31,32
- Obese Patients Have Significantly Higher Risk of Complications and Recurrence
- Treatment Approach:
- Overweight (BMI < 30): Elective Repair
- Obese (BMI 30-40): Elective Repair or Staged Repair
- Severely Obese (BMI > 40): Staged Repair
- Staged Repair:
- Start with Weight Loss by Bariatric Surgery or Multidisciplinary Medical Management
- Delay Hernia Repair Until Weight Loss is Achieved
- May Consider Combined Surgery (Hernia Repair and Bariatric Surgery) if Both are Amenable to Laparoscopic Repair for Severely Obese Patients 30
- Minimally Invasive Approaches are Generally Preferred – Decreased Risk of Wound Complications
Component Separation 33
- *See Abdominal Wall Reconstruction/Component Separation
- Indications:
- Multiple Defects Unable to Close with Mesh
- Large Defect Unable to Close Primarily
- Large Recurrence that Failed Suture Closure
- Giant Omphalocele
- Relative Contraindications:
- Extensive Destruction of Abdominal Wall Components
- Compromise of Epigastric Arterial Supply (DIEP Flap, etc.)
- Gross Contamination or Active Infection
Surgical Approach 34-37
- Choice of Approach is Often Surgeon Dependent with Minimally Invasive Techniques Evolving
- Open Surgery:
- Preferred for Small (< 1 cm) or Very Large (> 10 cm) Defects
- Preferred for Loss of Abdominal Domain
- Preferred if Bowel is Compromised with Necessary Resection – Incarceration Alone Can Be Done Laparoscopically
- Minimally Invasive (Laparoscopic or Robotic):
- Decreased Risk of Wound Complications – Particularly in Obese Patients
- Includes Hematoma, Seroma, and Surgical Site Infection
- Decreased Pain
- Decreased Length of Stay
- Provides Better Visualization for Multiple Defects (Avoids Larger-Than-Needed Incisions)
- Decreased Risk of Wound Complications – Particularly in Obese Patients
- Similar Recurrence Rates
- Robotic Repairs Have Longer Operative Times and Higher Costs
Special Populations
Hernia in Pediatrics
Umbilical Hernia in Pregnancy 38
- Asymptomatic: Observe
- Symptomatic: Delayed Repair After Delivery
- May Consider Elective Repair in the Second Trimester
- May Also Consider Concomitant Repair During C-Section
- Indications for Emergent Repair:
- Acutely Incarcerated
- Strangulated
- Skin Ulceration
Hernia with Ascites and Cirrhosis
References
- Mynter H. Reduction En Masse. Buffalo Med Surg J. 1888 Dec;28(5):245-250.
- Treves F. Richter’s Hernia or Partial Enterocele. Med Chir Trans. 1887;70:149-67.
- BARLING V. Interparietal hernia. Aust N Z J Surg. 1956 Aug;26(1):32-5.
- Pinto J, Viana CM, Pereira A, Falcão J. Littré’s hernia. BMJ Case Rep. 2019 Feb 28;12(2):e228784.
- Lee CH, Chien LJ, Shen CY, Su YJ. Amyand’s hernia. Am J Med Sci. 2022 Oct;364(4):e8-e9.
- Komorowski AL, Moran-Rodriguez J, Kazi R, Wysocki WM. Sliding inguinal hernias. Int J Surg. 2012;10(4):206-8.
- Henriksen NA, Montgomery A, Kaufmann R, Berrevoet F, East B, Fischer J, Hope W, Klassen D, Lorenz R, Renard Y, Garcia Urena MA, Simons MP; European and Americas Hernia Societies (EHS and AHS). Guidelines for treatment of umbilical and epigastric hernias from the European Hernia Society and Americas Hernia Society. Br J Surg. 2020 Feb;107(3):171-190.
- Waheed M, Alsenani M, Al-Akeely M, Al-Qahtani H. An unusual outcome of a giant ventral hernia. Saudi Med J. 2015 Aug;36(8):983-6. (License: CC BY-NC-SA 3.0)
- Abo-elmagd A, Ahmed K. Richter Paraumbilical Hernia Managed by Invagination: A Case Report and Review of Literature. Am J Surg Case Reports. 2019. (License: CC Unspecified)
- Elias B, Chelala E, Allé JL. Transabdominal Laparoscopic Repair of Amyand’s Hernia: A Case Report. Case Rep Surg. 2011;2011:823936. (License: CC BY 3.0)
- Nachiappan S, Markar S, Karthikesalingam A, Ziprin P, Faiz O. Prophylactic mesh placement in high-risk patients undergoing elective laparotomy: a systematic review. World J Surg. 2013 Aug;37(8):1861-71.
- Bucknall TE, Cox PJ, Ellis H. Burst abdomen and incisional hernia: a prospective study of 1129 major laparotomies. Br Med J (Clin Res Ed). 1982 Mar 27;284(6320):931-3.
- Sanders DL, Kingsnorth AN. The modern management of incisional hernias. BMJ. 2012 May 9;344:e2843.
- Bewö K, Österberg J, Löfgren M, Sandblom G. Incisional hernias following open gynecological surgery: a population-based study. Arch Gynecol Obstet. 2019 May;299(5):1313-1319.
- Oma E, Bay-Nielsen M, Jensen KK, Jorgensen LN, Pinborg A, Bisgaard T. Primary ventral or groin hernia in pregnancy: a cohort study of 20,714 women. Hernia(2017) 21(3):335–9.
- Reyna TM, Hollis HW Jr, Smith SB. Surgical management of proboscoid herniae. J Pediatr Surg. 1987 Oct;22(10):911-2.
- Ponten JE, Somers KY, Nienhuijs SW. Pathogenesis of the epigastric hernia. Hernia. 2012 Dec;16(6):627-33.
- Mittal T, Kumar V, Khullar R, Sharma A, Soni V, Baijal M, Chowbey PK. Diagnosis and management of Spigelian hernia: A review of literature and our experience. J Minim Access Surg. 2008 Oct;4(4):95-8. (License: CC BY 2.0)
- Cohen K, Kolwitz C, Petrone P, Halpern D. Arcuate line hernia: a case report. J Surg Case Rep. 2023 Feb 27;2023(2):rjad076.
- Cappeliez O, Duez V, Alle JL, Leclercq F. Bilateral arcuate-line hernia. AJR Am J Roentgenol. 2003 Mar;180(3):864-5. (License: CC BY-NC 4.0)
- Hammond E, Jones-Sayyid C, Langer J, Fox E, Lawson A. Posterior Rectus Sheath Hernia Causing Chronic Abdominal Pain. Am Surg. 2023 May 4:31348231173989.
- Wikimedia Commons (License: CC 1-1.0)
- Ashu EE, Leroy GM, Aristide BG, Joss BM, Bonaventure J, Patrick SE, Myriam FG. Double half-cone flap umbilicoplasty for proboscoid umbilical hernia in a 2 years old child with satisfactory results 2 years later. Pan Afr Med J. 2015 Sep 17;22:44. (License: CC BY 2.0)
- Wikimedia Commons (License: CC BY-SA 3.0)
- Ventral Hernia. Cleveland Clinic. 2018.
- Bosanquet DC, Ansell J, Abdelrahman T, Cornish J, Harries R, Stimpson A, Davies L, Glasbey JC, Frewer KA, Frewer NC, Russell D, Russell I, Torkington J. Systematic Review and Meta-Regression of Factors Affecting Midline Incisional Hernia Rates: Analysis of 14,618 Patients. PLoS One. 2015 Sep 21;10(9):e0138745.
- Walming S, Angenete E, Block M, Bock D, Gessler B, Haglind E. Retrospective review of risk factors for surgical wound dehiscence and incisional hernia. BMC Surg. 2017 Feb 22;17(1):19.
- Wikimedia Commons (License: Public Domain)
- Tao Z, Ordonez J, Huerta S. Hernia Size and Mesh Placement in Primary Umbilical Hernia Repair. Am Surg. 2021 Jun;87(6):1005-1013.
- Costantini TW, Martin D, Winchell R, Napolitano L, Inaba K, Biffl WL, Diaz JJ, Salim A, Livingston DH, Coimbra R. Evidence-based, cost-effective management of abdominal wall hernias: An algorithm of the Journal of Trauma and Acute Care Surgery emergency general surgery algorithms work group. J Trauma Acute Care Surg. 2025 May 1;98(5):692-698.
- Menzo EL, Hinojosa M, Carbonell A, Krpata D, Carter J, Rogers AM. American Society for Metabolic and Bariatric Surgery and American Hernia Society consensus guideline on bariatric surgery and hernia surgery. Surg Obes Relat Dis. 2018 Sep;14(9):1221-1232.
- Veilleux E, Lutfi R. Obesity and Ventral Hernia Repair: Is There Success in Staging? J Laparoendosc Adv Surg Tech A. 2020 Aug;30(8):896-899.
- Adekunle S, Pantelides NM, Hall NR, Praseedom R, Malata CM. Indications and outcomes of the components separation technique in the repair of complex abdominal wall hernias: experience from the cambridge plastic surgery department. Eplasty. 2013 Sep 16;13:e47.
- Zhang Y, Zhou H, Chai Y, Cao C, Jin K, Hu Z. Laparoscopic versus open incisional and ventral hernia repair: a systematic review and meta-analysis. World J Surg. 2014 Sep;38(9):2233-40.
- Al Chalabi H, Larkin J, Mehigan B, McCormick P. A systematic review of laparoscopic versus open abdominal incisional hernia repair, with meta-analysis of randomized controlled trials. Int J Surg. 2015 Aug;20:65-74.
- Sauerland S, Walgenbach M, Habermalz B, Seiler CM, Miserez M. Laparoscopic versus open surgical techniques for ventral or incisional hernia repair. Cochrane Database Syst Rev. 2011 Mar 16;(3):CD007781.
- Hajibandeh S, Hajibandeh S, Sreh A, Khan A, Subar D, Jones L. Laparoscopic versus open umbilical or paraumbilical hernia repair: a systematic review and meta-analysis. Hernia. 2017 Dec;21(6):905-916.
- Kulacoglu H. Umbilical Hernia Repair and Pregnancy: Before, during, after…. Front Surg. 2018 Jan 29;5:1.